Practical mental health commissioning: A framework for local authority and NHS commissioners of mental health and wellbeing services
the Joint Commissioning Panel for Mental Health in the UK
March 2011
Introduction
A comprehensive, strategic approach to improving mental health needs to include not only direct service provision for people currently experiencing and recovering from mental health problems, but also prevention and early intervention for those at high risk, and mental health promotion for the wider community.
Mental health describes a broad continuum of mental states that extends from mental illness, through mental ill health that may not reach the threshold for a formal diagnosis, to positive mental health and wellbeing. People will move in and out of these states throughout their life course, depending on a range of factors and influences, although most of us will not experience severe mental ill health.
Mental health is important at individual and family levels; it is no less important within communities and still more widely within our society as a whole. Interventions that improve the mental health of individuals will also improve the mental health of communities and promote and protect the mental health and resilience of the wider population. Better levels of mental health within the wider population also mean less severe mental illness, and better levels of support for those who are unwell.
Health and social care services are rising to the challenge to maximise quality and cost effectiveness in all service provision while also supporting individuals along their recovery journey. Increasingly, services are evidence-based and the people receiving these services are genuinely engaged in decision-making, not just at individual level but at organisational/strategic levels too. Personalisation is now the key principle that guides all care and treatment. Personalisation places the individual at the heart of decision-making, enabling them to make informed choices about the care and support they need to achieve the outcomes and goals they have identified and that are meaningful to them.
The framework
This framework is intended to guide commissioners as they traverse this complex and changing terrain.
The framework's main focus is on the mental health system, across all tiers, but it also addresses population mental health and health improvement, and the links between mental and physical health, especially for people with common and severe mental illnesses.
It takes an all-age approach, covering the whole of the life course from the very early years to old age. It does not delve in significant detail into children and young people's mental health and mental health in older age, but it will be supported by further, companion documents describing the key commissioning issues in these areas.
It explores the key policy imperatives driving commissioning for mental health into the future:
• improving population mental health and wellbeing and shifting the locus of power and responsibility to individuals, communities and local government
• increasing people's choice and control over services through personalisation of assessment processes and service provision
• system reform to support innovation and free up resources to follow people's choices through personalisation, Payment by Results (PbR) and related developments.
It describes the key commissioning enablers for achieving these three objectives. It seeks to knit into a coherent whole the multiple strands of improving quality, ensuring efficiency and productivity and supporting people to become more engaged in their own health care, while also managing increasing need and demand for services.
It recognises the multiplicity of factors involved in achieving quality and effectiveness in mental health and social care. Services need to be person-centred, cost-effective, clinically effective and safe. They have to work upstream, at the preventive and promotion end of the spectrum, as well as downstream with people experiencing severe mental illness. This requires commissioners to work in partnership across the public, independent, voluntary and community sectors, beyond the conventional boundaries of mental health provision.
1.4 Health and wellbeing boards
Local authorities will lead the strategic co-ordination of commissioning prevention and promotion (health and wellbeing) services further upstream, drawing together NHS, social care and related children's and public health services and working with other local agencies and groups. They will do this through health and wellbeing boards, which will be a statutory requirement in every upper tier authority.
The core purpose of the health and wellbeing boards is to join up commissioning across the NHS, social care, public health and other services that the board agrees have a direct influence in health and wellbeing, in order to secure better health and wellbeing outcomes for their whole population, better quality of care for users of health and social care services, and better value for the taxpayer.
The boards will provide the platform for NHS, public health and local authority leaders and commissioners to work together on a geographical basis, both within and between local authority areas.
The core membership of these boards will include all the GPCC covering that area, the director of adult social services, the director of children's services, the director of public health and the local HealthWatch (see below), and at least one locally elected member. Additional membership will be at the discretion of each board, but might include representatives of the local voluntary sector and other relevant public service officials, professionals and community organisations that can advise on and give voice to the needs of vulnerable and less-heard groups. Board membership might also include some providers, so long as this does not prejudice the level playing field within the local health and social care market.
Local authorities and the GPCC for their areas will undertake a joint strategic needs assessment through the health and wellbeing boards.
Health and wellbeing boards will also be the vehicle for the production of the new joint health and wellbeing strategies (JHWS). The JHWS is intended to provide the overarching framework for the development of the commissioning plans agreed by the health and wellbeing board for local NHS, social care, public health and other services. The JHWS could include wider health determinants such as housing and education.
GPCC and local authorities will have statutory responsibility for the production of both the JSNA and JHWS, and be required to pay regard to both in their commissioning plans, which must be approved by the health and wellbeing board. The boards will be expected to play an influential role in the development of innovative solutions to commissioning challenges, not simply to comment on commissioning plans.
Health and wellbeing boards will be able to look at the totality of resources available for health and wellbeing in their local area, and decide how to make best use of the flexibilities at their disposal, such as pooled budgets. Using the JHWS, they will be able to consider how prioritising health improvement and prevention, the management of long-term conditions and the provision of rehabilitation, recovery and re-ablement services will best deliver reductions in demand for health services and wider benefits for the health and wellbeing of the local population.
1.5 HealthWatch
Local authorities will retain their current health scrutiny powers, either through the existing health Overview and Scrutiny Committees (OSCs) or through other means if they choose. Local Involvement Networks (LINks) will evolve into local HealthWatch, supported and led by HealthWatch England. HealthWatch England will be based within the Care Quality Commission (CQC) and will act as an independent consumer champion. Local HealthWatch will ensure that the views of
1.6 Public health
Responsibility for public health, including public mental health, will be transferred to a new Public Health Service, Public Health England. This will be located within the Department of Health and will have its own ring-fenced budget. Directors of Public Health (DPH) will be located within local authorities, which will have responsibility for health improvement within their areas. The DPH will be expected to work with partner organisations - the NHS, the private, voluntary and public sectors and the GPCC - through the health and wellbeing board. Local authorities will receive a health premium to reward progress against the new public health outcomes framework.
Public health will be part of the NHS Commissioning Board's remit, and GPs potentially could receive enhanced incentives to deliver public health services.
1.7 Associated developments
Accompanying these major structural changes will be a number of other important developments in commissioning. These include:
• closer collaboration between primary and secondary care clinicians and professionals to enhance clinical leadership in commissioning. This collaboration should be built on the principles of integration and joint working in both commissioning and delivering a comprehensive mental health service across primary, secondary and social care sectors
• a major expansion of choice and involvement opportunities for individuals receiving primary, community and secondary care, with greater personalisation of services, increased freedom, choice and control and, crucially, a concentrated focus on improved health, public mental health and social care outcomes
• roll out of Payment by Results (PbR) for mental health services, and
• an imperative to achieve value for public money through QIPP and local government efficiency programmes, often predicated on economies of scale and joint or wider collaborative commissioning approaches.
1.8 Providers
On the provider side, there will be a continued move away from central control, with greater autonomy for NHS Foundation Trusts and greater opportunities for more, and larger, social enterprises to move into direct health and social care provision. The aim is to free up providers so that they can compete on a level playing field, focus on improving outcomes, be more responsive to the needs of people using services, and innovate.
This process will be facilitated by the 'any willing provider' concept outlined above.
Praktyczne zamawianie zdrowia psychicznego: Ramy dla władz lokalnych i pełnomocników NHS ds. usług w zakresie zdrowia psychicznego i dobrego samopoczucia
Wspólny Panel Zlecający ds. Zdrowia Psychicznego w Wielkiej Brytanii
Marzec 2011
Wstęp
Kompleksowe, strategiczne podejście do poprawy zdrowia psychicznego musi obejmować nie tylko bezpośrednie świadczenie usług osobom obecnie doświadczającym problemów psychicznych i wracających do zdrowia po problemach psychicznych, ale także profilaktykę i wczesną interwencję dla osób z grupy wysokiego ryzyka oraz promocję zdrowia psychicznego w szerszej społeczności.
Zdrowie psychiczne opisuje szerokie kontinuum stanów psychicznych, które rozciąga się od choroby psychicznej, przez zły stan zdrowia psychicznego, który może nie osiągnąć progu formalnej diagnozy, aż do pozytywnego zdrowia psychicznego i dobrego samopoczucia. Ludzie będą wprowadzać się i wyjeżdżać z tych stanów przez całe życie, w zależności od szeregu czynników i wpływów, chociaż większość z nas nie doświadczy poważnych problemów psychicznych.
Zdrowie psychiczne jest ważne na poziomie indywidualnym i rodzinnym; jest nie mniej ważny w obrębie społeczności, a jeszcze szerzej – w naszym społeczeństwie jako całości. Interwencje poprawiające zdrowie psychiczne jednostek poprawią również zdrowie psychiczne społeczności oraz będą promować i chronić zdrowie psychiczne i odporność szerszej populacji. Lepszy poziom zdrowia psychicznego w szerszej populacji oznacza także mniej poważne choroby psychiczne i lepszy poziom wsparcia dla osób chorych.
Służby zdrowia i opieki społecznej podejmują wyzwanie maksymalizacji jakości i efektywności kosztowej wszystkich świadczonych usług, jednocześnie wspierając osoby na drodze do powrotu do zdrowia. Usługi w coraz większym stopniu opierają się na dowodach, a osoby korzystające z tych usług są rzeczywiście zaangażowane w podejmowanie decyzji, nie tylko na poziomie indywidualnym, ale także na poziomie organizacyjnym /strategicznym. Personalizacja jest obecnie kluczową zasadą, która kieruje całą opieką i leczeniem. Personalizacja stawia jednostkę w centrum procesu decyzyjnego, umożliwiając jej podejmowanie świadomych wyborów dotyczących opieki i wsparcia, których potrzebuje, aby osiągnąć określone przez siebie wyniki i cele, które są dla niej znaczące.
Ramy
Ramy te mają służyć jako wskazówki dla komisarzy podczas przemierzania tego złożonego i zmieniającego się terenu.
Ramy skupiają się głównie na systemie zdrowia psychicznego na wszystkich poziomach, ale uwzględniają także zdrowie psychiczne populacji i poprawę zdrowia oraz powiązania między zdrowiem psychicznym i fizycznym, szczególnie w przypadku osób cierpiących na powszechne i poważne choroby psychiczne.
Wymaga podejścia uwzględniającego cały wiek, obejmującego cały cykl życia, od najmłodszych lat do starości. Nie zagłębia się w szczegóły zdrowia psychicznego dzieci i młodych ludzi oraz zdrowia psychicznego w starszym wieku, ale będzie poparte dalszymi dokumentami towarzyszącymi opisującymi kluczowe kwestie związane z uruchomieniem w tych obszarach.
Bada kluczowe imperatywy polityczne, które będą napędzać w przyszłości zlecanie działań w zakresie zdrowia psychicznego:
• poprawa zdrowia psychicznego i dobrostanu populacji oraz przeniesienie umiejscowienia władzy i odpowiedzialności na jednostki, społeczności i władze lokalne
• zwiększanie wyboru ludzi i kontroli nad usługami poprzez personalizację procesów oceny i świadczenia usług
• reforma systemu mająca na celu wspieranie innowacji i uwolnienie zasobów umożliwiających podążanie za wyborami ludzi poprzez personalizację, płatność według wyników ( PbR ) i powiązane zmiany.
Opisuje kluczowe czynniki umożliwiające osiągnięcie tych trzech celów podczas uruchamiania. Ma na celu połączenie w spójną całość wielu aspektów poprawy jakości, zapewnienia wydajności i produktywności oraz wspierania ludzi w większym zaangażowaniu się we własną opiekę zdrowotną, przy jednoczesnym zarządzaniu rosnącym zapotrzebowaniem i popytem na usługi.
Uznaje wielość czynników wpływających na osiągnięcie jakości i skuteczności w zakresie zdrowia psychicznego i opieki społecznej. Usługi muszą być skoncentrowane na osobie, opłacalne, skuteczne klinicznie i bezpieczne. Muszą pracować od początku, na końcu spektrum w zakresie profilaktyki i promocji, a także od dołu do góry, z osobami doświadczającymi poważnych chorób psychicznych. Wymaga to od komisarzy partnerskiej współpracy w sektorach publicznym, niezależnym, wolontariackim i społecznym, wykraczającym poza konwencjonalne granice zapewniania zdrowia psychicznego.
1.4 Tablice zdrowia i dobrego samopoczucia
Władze lokalne będą kierować strategiczną koordynacją zlecania usług w zakresie profilaktyki i promocji (zdrowia i dobrego samopoczucia) na dalszych etapach łańcucha dostaw, łącząc NHS, opiekę społeczną i powiązane usługi na rzecz dzieci i zdrowia publicznego oraz współpracując z innymi lokalnymi agencjami i grupami. Zrobią to za pośrednictwem rad ds. zdrowia i dobrego samopoczucia, co będzie wymogiem ustawowym wszystkich organów wyższego szczebla.
Podstawowym celem rad ds. zdrowia i dobrego samopoczucia jest łączenie podmiotów świadczących usługi w ramach NHS, opieki społecznej, zdrowia publicznego i innych usług, które zdaniem rady mają bezpośredni wpływ na zdrowie i dobre samopoczucie, w celu zapewnienia swoim pracownikom lepszych wyników w zakresie zdrowia i dobrostanu. całej populacji, lepszą jakość opieki dla osób korzystających z usług opieki zdrowotnej i społecznej oraz lepszą wartość dla podatnika.
Rady zapewnią platformę dla liderów i komisarzy NHS, zdrowia publicznego i władz lokalnych, umożliwiającą współpracę na podstawie geograficznej, zarówno w obrębie obszarów władz lokalnych, jak i pomiędzy nimi.
Do głównych członków tych rad należeć będą wszystkie GPCC działające na tym obszarze, dyrektor ds. usług socjalnych dla dorosłych, dyrektor ds. usług dla dzieci, dyrektor ds. zdrowia publicznego i lokalnego HealthWatch (patrz poniżej) oraz co najmniej jeden członek wybrany lokalnie. Dodatkowe członkostwo będzie zależało od uznania każdego zarządu, ale może obejmować przedstawicieli lokalnego sektora wolontariatu i innych odpowiednich urzędników służby publicznej, specjalistów i organizacje społeczne, które mogą doradzać i wyrażać potrzeby grup bezbronnych i mniej słyszanych. Członkami Zarządu mogą być także niektórzy świadczeniodawcy, o ile nie narusza to równych warunków działania na lokalnym rynku opieki zdrowotnej i społecznej.
Władze lokalne i GPCC na swoich obszarach przeprowadzą wspólną ocenę potrzeb strategicznych za pośrednictwem rad ds. zdrowia i dobrego samopoczucia.
Rady ds. zdrowia i dobrego samopoczucia będą także narzędziem do tworzenia nowych wspólnych strategii na rzecz zdrowia i dobrego samopoczucia (JHWS). JHWS ma zapewnić nadrzędne ramy dla opracowywania planów uruchomienia uzgodnionych przez radę ds. zdrowia i dobrego samopoczucia dla lokalnej NHS, opieki społecznej, zdrowia publicznego i innych usług. JHWS mógłby obejmować szersze czynniki warunkujące zdrowie, takie jak mieszkalnictwo i edukacja.
GPCC i władze lokalne będą ponosić ustawową odpowiedzialność za produkcję zarówno JSNA, jak i JHWS i będą zobowiązane do uwzględnienia obu w swoich planach uruchomienia, które muszą zostać zatwierdzone przez radę ds. zdrowia i dobrego samopoczucia. Oczekuje się, że rady odegrają wpływową rolę w opracowywaniu innowacyjnych rozwiązań problemów związanych z oddaniem do użytku, a nie tylko będą komentować plany oddania do użytku.
Rady ds. zdrowia i dobrego samopoczucia będą mogły przyjrzeć się całości zasobów dostępnych na rzecz zdrowia i dobrego samopoczucia na swoim obszarze lokalnym i zdecydować, w jaki sposób najlepiej wykorzystać dostępne im możliwości elastyczności, takie jak wspólne budżety. Korzystając z JHWS, będą mogli rozważyć, w jaki sposób nadanie priorytetu poprawie zdrowia i profilaktyce, zarządzaniu długoterminowymi schorzeniami oraz zapewnieniu usług rehabilitacyjnych, rekonwalescencji i przywracania sprawności najlepiej zapewni zmniejszenie popytu na usługi zdrowotne i szersze korzyści dla społeczeństwa zdrowie i dobre samopoczucie lokalnej ludności.
1.5 Zegarek zdrowia
Władze lokalne zachowają swoje obecne uprawnienia w zakresie kontroli stanu zdrowia za pośrednictwem istniejących komisji ds. przeglądu i kontroli stanu zdrowia (OSC) lub w inny sposób, jeśli tak zdecydują. Lokalne sieci zaangażowania ( LINKs ) przekształcą się w lokalną organizację HealthWatch , wspieraną i prowadzoną przez HealthWatch England. Organizacja HealthWatch England będzie działać w ramach Komisji ds. Jakości Opieki (CQC) i będzie działać jako niezależny orędownik konsumencki. Lokalna organizacja HealthWatch zadba o to, aby poglądy:
1.6 Zdrowie publiczne
Odpowiedzialność za zdrowie publiczne, w tym publiczne zdrowie psychiczne, zostanie przeniesiona na nową służbę zdrowia publicznego, Public Health England. Będzie ono zlokalizowane w Departamencie Zdrowia i będzie dysponowało własnym, wyodrębnionym budżetem. Dyrektorzy ds. zdrowia publicznego (DPH) będą zlokalizowani we władzach lokalnych, które będą odpowiedzialne za poprawę zdrowia na swoich obszarach. Oczekuje się, że DPH będzie współpracować z organizacjami partnerskimi – NHS, sektorem prywatnym, wolontariackim i publicznym oraz GPCC – za pośrednictwem rady ds. zdrowia i dobrego samopoczucia. Władze lokalne otrzymają premię zdrowotną w ramach nagrody za postępy w realizacji nowych ram dotyczących wyników w zakresie zdrowia publicznego.
Zdrowie publiczne będzie częścią kompetencji Rady ds. Zleceń NHS, a lekarze pierwszego kontaktu mogliby potencjalnie otrzymać zwiększone zachęty do świadczenia publicznych usług zdrowotnych.
1.7 Powiązane zmiany
Tym poważnym zmianom strukturalnym będzie towarzyszyć szereg innych ważnych zmian w zakresie oddania do eksploatacji. Obejmują one:
• bliższa współpraca między lekarzami i specjalistami zajmującymi się opieką podstawową i specjalistyczną w celu wzmocnienia przywództwa klinicznego w zakresie zlecania leczenia. Współpraca ta powinna opierać się na zasadach integracji i wspólnej pracy zarówno przy zlecaniu, jak i świadczeniu kompleksowych usług w zakresie zdrowia psychicznego w sektorach opieki podstawowej, średniej i społecznej
• znaczne poszerzenie możliwości wyboru i zaangażowania dla osób korzystających z opieki podstawowej, środowiskowej i specjalistycznej, z większą personalizacją usług, większą swobodą, wyborem i kontrolą oraz, co najważniejsze, skoncentrowanym naciskiem na poprawę zdrowia, publicznego zdrowia psychicznego i wyników opieki społecznej
• wprowadzenie płatności według wyników ( PbR ) dla usług w zakresie zdrowia psychicznego oraz
• konieczność osiągnięcia wartości za publiczne pieniądze poprzez QIPP i programy efektywności samorządów lokalnych , często opierające się na korzyściach skali i podejściu do zlecania zamówień na zasadzie wspólnej lub szerszej współpracy.
1.8 Dostawcy
Po stronie świadczeniodawców będzie następowało ciągłe odchodzenie od kontroli centralnej, co zapewni większą autonomię fundacji NHS Foundation Trust i większe możliwości dla większej liczby większych przedsiębiorstw społecznych w zakresie bezpośredniego świadczenia opieki zdrowotnej i społecznej. Celem jest uwolnienie dostawców, aby mogli konkurować na równych warunkach, skoncentrować się na poprawie wyników, lepiej reagować na potrzeby osób korzystających z usług i wprowadzać innowacje.
Proces ten ułatwi opisana powyżej koncepcja „każdego chętnego dostawcy”.
the Joint Commissioning Panel for Mental Health in the UK
March 2011
Introduction
A comprehensive, strategic approach to improving mental health needs to include not only direct service provision for people currently experiencing and recovering from mental health problems, but also prevention and early intervention for those at high risk, and mental health promotion for the wider community.
Mental health describes a broad continuum of mental states that extends from mental illness, through mental ill health that may not reach the threshold for a formal diagnosis, to positive mental health and wellbeing. People will move in and out of these states throughout their life course, depending on a range of factors and influences, although most of us will not experience severe mental ill health.
Mental health is important at individual and family levels; it is no less important within communities and still more widely within our society as a whole. Interventions that improve the mental health of individuals will also improve the mental health of communities and promote and protect the mental health and resilience of the wider population. Better levels of mental health within the wider population also mean less severe mental illness, and better levels of support for those who are unwell.
Health and social care services are rising to the challenge to maximise quality and cost effectiveness in all service provision while also supporting individuals along their recovery journey. Increasingly, services are evidence-based and the people receiving these services are genuinely engaged in decision-making, not just at individual level but at organisational/strategic levels too. Personalisation is now the key principle that guides all care and treatment. Personalisation places the individual at the heart of decision-making, enabling them to make informed choices about the care and support they need to achieve the outcomes and goals they have identified and that are meaningful to them.
The framework
This framework is intended to guide commissioners as they traverse this complex and changing terrain.
The framework's main focus is on the mental health system, across all tiers, but it also addresses population mental health and health improvement, and the links between mental and physical health, especially for people with common and severe mental illnesses.
It takes an all-age approach, covering the whole of the life course from the very early years to old age. It does not delve in significant detail into children and young people's mental health and mental health in older age, but it will be supported by further, companion documents describing the key commissioning issues in these areas.
It explores the key policy imperatives driving commissioning for mental health into the future:
• improving population mental health and wellbeing and shifting the locus of power and responsibility to individuals, communities and local government
• increasing people's choice and control over services through personalisation of assessment processes and service provision
• system reform to support innovation and free up resources to follow people's choices through personalisation, Payment by Results (PbR) and related developments.
It describes the key commissioning enablers for achieving these three objectives. It seeks to knit into a coherent whole the multiple strands of improving quality, ensuring efficiency and productivity and supporting people to become more engaged in their own health care, while also managing increasing need and demand for services.
It recognises the multiplicity of factors involved in achieving quality and effectiveness in mental health and social care. Services need to be person-centred, cost-effective, clinically effective and safe. They have to work upstream, at the preventive and promotion end of the spectrum, as well as downstream with people experiencing severe mental illness. This requires commissioners to work in partnership across the public, independent, voluntary and community sectors, beyond the conventional boundaries of mental health provision.
1.4 Health and wellbeing boards
Local authorities will lead the strategic co-ordination of commissioning prevention and promotion (health and wellbeing) services further upstream, drawing together NHS, social care and related children's and public health services and working with other local agencies and groups. They will do this through health and wellbeing boards, which will be a statutory requirement in every upper tier authority.
The core purpose of the health and wellbeing boards is to join up commissioning across the NHS, social care, public health and other services that the board agrees have a direct influence in health and wellbeing, in order to secure better health and wellbeing outcomes for their whole population, better quality of care for users of health and social care services, and better value for the taxpayer.
The boards will provide the platform for NHS, public health and local authority leaders and commissioners to work together on a geographical basis, both within and between local authority areas.
The core membership of these boards will include all the GPCC covering that area, the director of adult social services, the director of children's services, the director of public health and the local HealthWatch (see below), and at least one locally elected member. Additional membership will be at the discretion of each board, but might include representatives of the local voluntary sector and other relevant public service officials, professionals and community organisations that can advise on and give voice to the needs of vulnerable and less-heard groups. Board membership might also include some providers, so long as this does not prejudice the level playing field within the local health and social care market.
Local authorities and the GPCC for their areas will undertake a joint strategic needs assessment through the health and wellbeing boards.
Health and wellbeing boards will also be the vehicle for the production of the new joint health and wellbeing strategies (JHWS). The JHWS is intended to provide the overarching framework for the development of the commissioning plans agreed by the health and wellbeing board for local NHS, social care, public health and other services. The JHWS could include wider health determinants such as housing and education.
GPCC and local authorities will have statutory responsibility for the production of both the JSNA and JHWS, and be required to pay regard to both in their commissioning plans, which must be approved by the health and wellbeing board. The boards will be expected to play an influential role in the development of innovative solutions to commissioning challenges, not simply to comment on commissioning plans.
Health and wellbeing boards will be able to look at the totality of resources available for health and wellbeing in their local area, and decide how to make best use of the flexibilities at their disposal, such as pooled budgets. Using the JHWS, they will be able to consider how prioritising health improvement and prevention, the management of long-term conditions and the provision of rehabilitation, recovery and re-ablement services will best deliver reductions in demand for health services and wider benefits for the health and wellbeing of the local population.
1.5 HealthWatch
Local authorities will retain their current health scrutiny powers, either through the existing health Overview and Scrutiny Committees (OSCs) or through other means if they choose. Local Involvement Networks (LINks) will evolve into local HealthWatch, supported and led by HealthWatch England. HealthWatch England will be based within the Care Quality Commission (CQC) and will act as an independent consumer champion. Local HealthWatch will ensure that the views of
1.6 Public health
Responsibility for public health, including public mental health, will be transferred to a new Public Health Service, Public Health England. This will be located within the Department of Health and will have its own ring-fenced budget. Directors of Public Health (DPH) will be located within local authorities, which will have responsibility for health improvement within their areas. The DPH will be expected to work with partner organisations - the NHS, the private, voluntary and public sectors and the GPCC - through the health and wellbeing board. Local authorities will receive a health premium to reward progress against the new public health outcomes framework.
Public health will be part of the NHS Commissioning Board's remit, and GPs potentially could receive enhanced incentives to deliver public health services.
1.7 Associated developments
Accompanying these major structural changes will be a number of other important developments in commissioning. These include:
• closer collaboration between primary and secondary care clinicians and professionals to enhance clinical leadership in commissioning. This collaboration should be built on the principles of integration and joint working in both commissioning and delivering a comprehensive mental health service across primary, secondary and social care sectors
• a major expansion of choice and involvement opportunities for individuals receiving primary, community and secondary care, with greater personalisation of services, increased freedom, choice and control and, crucially, a concentrated focus on improved health, public mental health and social care outcomes
• roll out of Payment by Results (PbR) for mental health services, and
• an imperative to achieve value for public money through QIPP and local government efficiency programmes, often predicated on economies of scale and joint or wider collaborative commissioning approaches.
1.8 Providers
On the provider side, there will be a continued move away from central control, with greater autonomy for NHS Foundation Trusts and greater opportunities for more, and larger, social enterprises to move into direct health and social care provision. The aim is to free up providers so that they can compete on a level playing field, focus on improving outcomes, be more responsive to the needs of people using services, and innovate.
This process will be facilitated by the 'any willing provider' concept outlined above.
Praktyczne zamawianie zdrowia psychicznego: Ramy dla władz lokalnych i pełnomocników NHS ds. usług w zakresie zdrowia psychicznego i dobrego samopoczucia
Wspólny Panel Zlecający ds. Zdrowia Psychicznego w Wielkiej Brytanii
Marzec 2011
Wstęp
Kompleksowe, strategiczne podejście do poprawy zdrowia psychicznego musi obejmować nie tylko bezpośrednie świadczenie usług osobom obecnie doświadczającym problemów psychicznych i wracających do zdrowia po problemach psychicznych, ale także profilaktykę i wczesną interwencję dla osób z grupy wysokiego ryzyka oraz promocję zdrowia psychicznego w szerszej społeczności.
Zdrowie psychiczne opisuje szerokie kontinuum stanów psychicznych, które rozciąga się od choroby psychicznej, przez zły stan zdrowia psychicznego, który może nie osiągnąć progu formalnej diagnozy, aż do pozytywnego zdrowia psychicznego i dobrego samopoczucia. Ludzie będą wprowadzać się i wyjeżdżać z tych stanów przez całe życie, w zależności od szeregu czynników i wpływów, chociaż większość z nas nie doświadczy poważnych problemów psychicznych.
Zdrowie psychiczne jest ważne na poziomie indywidualnym i rodzinnym; jest nie mniej ważny w obrębie społeczności, a jeszcze szerzej – w naszym społeczeństwie jako całości. Interwencje poprawiające zdrowie psychiczne jednostek poprawią również zdrowie psychiczne społeczności oraz będą promować i chronić zdrowie psychiczne i odporność szerszej populacji. Lepszy poziom zdrowia psychicznego w szerszej populacji oznacza także mniej poważne choroby psychiczne i lepszy poziom wsparcia dla osób chorych.
Służby zdrowia i opieki społecznej podejmują wyzwanie maksymalizacji jakości i efektywności kosztowej wszystkich świadczonych usług, jednocześnie wspierając osoby na drodze do powrotu do zdrowia. Usługi w coraz większym stopniu opierają się na dowodach, a osoby korzystające z tych usług są rzeczywiście zaangażowane w podejmowanie decyzji, nie tylko na poziomie indywidualnym, ale także na poziomie organizacyjnym /strategicznym. Personalizacja jest obecnie kluczową zasadą, która kieruje całą opieką i leczeniem. Personalizacja stawia jednostkę w centrum procesu decyzyjnego, umożliwiając jej podejmowanie świadomych wyborów dotyczących opieki i wsparcia, których potrzebuje, aby osiągnąć określone przez siebie wyniki i cele, które są dla niej znaczące.
Ramy
Ramy te mają służyć jako wskazówki dla komisarzy podczas przemierzania tego złożonego i zmieniającego się terenu.
Ramy skupiają się głównie na systemie zdrowia psychicznego na wszystkich poziomach, ale uwzględniają także zdrowie psychiczne populacji i poprawę zdrowia oraz powiązania między zdrowiem psychicznym i fizycznym, szczególnie w przypadku osób cierpiących na powszechne i poważne choroby psychiczne.
Wymaga podejścia uwzględniającego cały wiek, obejmującego cały cykl życia, od najmłodszych lat do starości. Nie zagłębia się w szczegóły zdrowia psychicznego dzieci i młodych ludzi oraz zdrowia psychicznego w starszym wieku, ale będzie poparte dalszymi dokumentami towarzyszącymi opisującymi kluczowe kwestie związane z uruchomieniem w tych obszarach.
Bada kluczowe imperatywy polityczne, które będą napędzać w przyszłości zlecanie działań w zakresie zdrowia psychicznego:
• poprawa zdrowia psychicznego i dobrostanu populacji oraz przeniesienie umiejscowienia władzy i odpowiedzialności na jednostki, społeczności i władze lokalne
• zwiększanie wyboru ludzi i kontroli nad usługami poprzez personalizację procesów oceny i świadczenia usług
• reforma systemu mająca na celu wspieranie innowacji i uwolnienie zasobów umożliwiających podążanie za wyborami ludzi poprzez personalizację, płatność według wyników ( PbR ) i powiązane zmiany.
Opisuje kluczowe czynniki umożliwiające osiągnięcie tych trzech celów podczas uruchamiania. Ma na celu połączenie w spójną całość wielu aspektów poprawy jakości, zapewnienia wydajności i produktywności oraz wspierania ludzi w większym zaangażowaniu się we własną opiekę zdrowotną, przy jednoczesnym zarządzaniu rosnącym zapotrzebowaniem i popytem na usługi.
Uznaje wielość czynników wpływających na osiągnięcie jakości i skuteczności w zakresie zdrowia psychicznego i opieki społecznej. Usługi muszą być skoncentrowane na osobie, opłacalne, skuteczne klinicznie i bezpieczne. Muszą pracować od początku, na końcu spektrum w zakresie profilaktyki i promocji, a także od dołu do góry, z osobami doświadczającymi poważnych chorób psychicznych. Wymaga to od komisarzy partnerskiej współpracy w sektorach publicznym, niezależnym, wolontariackim i społecznym, wykraczającym poza konwencjonalne granice zapewniania zdrowia psychicznego.
1.4 Tablice zdrowia i dobrego samopoczucia
Władze lokalne będą kierować strategiczną koordynacją zlecania usług w zakresie profilaktyki i promocji (zdrowia i dobrego samopoczucia) na dalszych etapach łańcucha dostaw, łącząc NHS, opiekę społeczną i powiązane usługi na rzecz dzieci i zdrowia publicznego oraz współpracując z innymi lokalnymi agencjami i grupami. Zrobią to za pośrednictwem rad ds. zdrowia i dobrego samopoczucia, co będzie wymogiem ustawowym wszystkich organów wyższego szczebla.
Podstawowym celem rad ds. zdrowia i dobrego samopoczucia jest łączenie podmiotów świadczących usługi w ramach NHS, opieki społecznej, zdrowia publicznego i innych usług, które zdaniem rady mają bezpośredni wpływ na zdrowie i dobre samopoczucie, w celu zapewnienia swoim pracownikom lepszych wyników w zakresie zdrowia i dobrostanu. całej populacji, lepszą jakość opieki dla osób korzystających z usług opieki zdrowotnej i społecznej oraz lepszą wartość dla podatnika.
Rady zapewnią platformę dla liderów i komisarzy NHS, zdrowia publicznego i władz lokalnych, umożliwiającą współpracę na podstawie geograficznej, zarówno w obrębie obszarów władz lokalnych, jak i pomiędzy nimi.
Do głównych członków tych rad należeć będą wszystkie GPCC działające na tym obszarze, dyrektor ds. usług socjalnych dla dorosłych, dyrektor ds. usług dla dzieci, dyrektor ds. zdrowia publicznego i lokalnego HealthWatch (patrz poniżej) oraz co najmniej jeden członek wybrany lokalnie. Dodatkowe członkostwo będzie zależało od uznania każdego zarządu, ale może obejmować przedstawicieli lokalnego sektora wolontariatu i innych odpowiednich urzędników służby publicznej, specjalistów i organizacje społeczne, które mogą doradzać i wyrażać potrzeby grup bezbronnych i mniej słyszanych. Członkami Zarządu mogą być także niektórzy świadczeniodawcy, o ile nie narusza to równych warunków działania na lokalnym rynku opieki zdrowotnej i społecznej.
Władze lokalne i GPCC na swoich obszarach przeprowadzą wspólną ocenę potrzeb strategicznych za pośrednictwem rad ds. zdrowia i dobrego samopoczucia.
Rady ds. zdrowia i dobrego samopoczucia będą także narzędziem do tworzenia nowych wspólnych strategii na rzecz zdrowia i dobrego samopoczucia (JHWS). JHWS ma zapewnić nadrzędne ramy dla opracowywania planów uruchomienia uzgodnionych przez radę ds. zdrowia i dobrego samopoczucia dla lokalnej NHS, opieki społecznej, zdrowia publicznego i innych usług. JHWS mógłby obejmować szersze czynniki warunkujące zdrowie, takie jak mieszkalnictwo i edukacja.
GPCC i władze lokalne będą ponosić ustawową odpowiedzialność za produkcję zarówno JSNA, jak i JHWS i będą zobowiązane do uwzględnienia obu w swoich planach uruchomienia, które muszą zostać zatwierdzone przez radę ds. zdrowia i dobrego samopoczucia. Oczekuje się, że rady odegrają wpływową rolę w opracowywaniu innowacyjnych rozwiązań problemów związanych z oddaniem do użytku, a nie tylko będą komentować plany oddania do użytku.
Rady ds. zdrowia i dobrego samopoczucia będą mogły przyjrzeć się całości zasobów dostępnych na rzecz zdrowia i dobrego samopoczucia na swoim obszarze lokalnym i zdecydować, w jaki sposób najlepiej wykorzystać dostępne im możliwości elastyczności, takie jak wspólne budżety. Korzystając z JHWS, będą mogli rozważyć, w jaki sposób nadanie priorytetu poprawie zdrowia i profilaktyce, zarządzaniu długoterminowymi schorzeniami oraz zapewnieniu usług rehabilitacyjnych, rekonwalescencji i przywracania sprawności najlepiej zapewni zmniejszenie popytu na usługi zdrowotne i szersze korzyści dla społeczeństwa zdrowie i dobre samopoczucie lokalnej ludności.
1.5 Zegarek zdrowia
Władze lokalne zachowają swoje obecne uprawnienia w zakresie kontroli stanu zdrowia za pośrednictwem istniejących komisji ds. przeglądu i kontroli stanu zdrowia (OSC) lub w inny sposób, jeśli tak zdecydują. Lokalne sieci zaangażowania ( LINKs ) przekształcą się w lokalną organizację HealthWatch , wspieraną i prowadzoną przez HealthWatch England. Organizacja HealthWatch England będzie działać w ramach Komisji ds. Jakości Opieki (CQC) i będzie działać jako niezależny orędownik konsumencki. Lokalna organizacja HealthWatch zadba o to, aby poglądy:
1.6 Zdrowie publiczne
Odpowiedzialność za zdrowie publiczne, w tym publiczne zdrowie psychiczne, zostanie przeniesiona na nową służbę zdrowia publicznego, Public Health England. Będzie ono zlokalizowane w Departamencie Zdrowia i będzie dysponowało własnym, wyodrębnionym budżetem. Dyrektorzy ds. zdrowia publicznego (DPH) będą zlokalizowani we władzach lokalnych, które będą odpowiedzialne za poprawę zdrowia na swoich obszarach. Oczekuje się, że DPH będzie współpracować z organizacjami partnerskimi – NHS, sektorem prywatnym, wolontariackim i publicznym oraz GPCC – za pośrednictwem rady ds. zdrowia i dobrego samopoczucia. Władze lokalne otrzymają premię zdrowotną w ramach nagrody za postępy w realizacji nowych ram dotyczących wyników w zakresie zdrowia publicznego.
Zdrowie publiczne będzie częścią kompetencji Rady ds. Zleceń NHS, a lekarze pierwszego kontaktu mogliby potencjalnie otrzymać zwiększone zachęty do świadczenia publicznych usług zdrowotnych.
1.7 Powiązane zmiany
Tym poważnym zmianom strukturalnym będzie towarzyszyć szereg innych ważnych zmian w zakresie oddania do eksploatacji. Obejmują one:
• bliższa współpraca między lekarzami i specjalistami zajmującymi się opieką podstawową i specjalistyczną w celu wzmocnienia przywództwa klinicznego w zakresie zlecania leczenia. Współpraca ta powinna opierać się na zasadach integracji i wspólnej pracy zarówno przy zlecaniu, jak i świadczeniu kompleksowych usług w zakresie zdrowia psychicznego w sektorach opieki podstawowej, średniej i społecznej
• znaczne poszerzenie możliwości wyboru i zaangażowania dla osób korzystających z opieki podstawowej, środowiskowej i specjalistycznej, z większą personalizacją usług, większą swobodą, wyborem i kontrolą oraz, co najważniejsze, skoncentrowanym naciskiem na poprawę zdrowia, publicznego zdrowia psychicznego i wyników opieki społecznej
• wprowadzenie płatności według wyników ( PbR ) dla usług w zakresie zdrowia psychicznego oraz
• konieczność osiągnięcia wartości za publiczne pieniądze poprzez QIPP i programy efektywności samorządów lokalnych , często opierające się na korzyściach skali i podejściu do zlecania zamówień na zasadzie wspólnej lub szerszej współpracy.
1.8 Dostawcy
Po stronie świadczeniodawców będzie następowało ciągłe odchodzenie od kontroli centralnej, co zapewni większą autonomię fundacji NHS Foundation Trust i większe możliwości dla większej liczby większych przedsiębiorstw społecznych w zakresie bezpośredniego świadczenia opieki zdrowotnej i społecznej. Celem jest uwolnienie dostawców, aby mogli konkurować na równych warunkach, skoncentrować się na poprawie wyników, lepiej reagować na potrzeby osób korzystających z usług i wprowadzać innowacje.
Proces ten ułatwi opisana powyżej koncepcja „każdego chętnego dostawcy”.
PAYMENT BY RESULTS IN MENTAL HEALTH - THE CURRENT STATE OF PLAY IN ENGLAND
Andrew Fairbairn
Advances in Psychiatric Treatment (2007), vol. 13, 3–6 doi
https://www.cambridge.org/core/journals/advances-in-psychiatric-treatment/article/payment-by-results-in-mental-health-the-current-state-of-play-in-england/AA2E5C377A46E4019604924D28D24522
Abstract
The Department of Health is introducing a 'payment by results' system for mental health services in the UK. The system is already being used in the acute healthcare sector, but is still under development for application in mental healthcare. This article outlines the concept of payment by results, briefly reports on its use in other countries and describes the pilot study underway in England to define currencies to be used in a payment by results system planned for NHS mental healthcare throughout England and Wales.
‘Payment by results’ is a method of paying for the services of hospitals and other providers. Plans are well underway to use it within the National Health Service (NHS) in England, and some health authorities began to introduce it in 2005. The discussion of payment by results is usually peppered with abbreviations. I have used these only rarely in this article, but a list of those most commonly encountered in the literature appears.
Payment by results has three central components.
The first is activity-based funding, which contrasts with the more traditional block contract agreements. For service providers, more work will generate more income or, indeed, less work will generate less.
Second, the amount of work tends to be measured in the context of healthcare resource groups. These are groupings of individual cases that are sufficiently clinically similar and require similar treatment resources. In the acute healthcare sector they tend to be based on international categories of diagnosis. They also take into account procedures, complications and co-existing illnesses. Therefore any payment by results system seeks to provide a coherent manageable way of classifying the mixed cases treated within a hospital. This is why payment by results is sometimes called a system of case-mixed funding.
Third, payment is made according to a national tariff. This tariff is a price tag for any individual healthcare resource group. The price tends to be based on the average cost of treatment across the NHS. This national tariff means that contractual negotiations between commissioners and providers no longer require price negotiation but can concentrate on quantity and quality of care.
It is important to recognise that a number of countries have investigated the possibility of a payment by results system and none so far has successfully implemented such a scheme. Some results of studies in Australia and New Zealand are briefly discussed below but one must draw the conclusion that there maybe a message in this. Nevertheless, the system has been introduced in most of the acute sector of the NHS in England and the Department of Health has put pressure on service commissioners to use it. There is anecdotal evidence that, as the system has not yet been implemented in the mental health sector, commissioners have taken the opportunity to squeeze mental health service funding in order to meet cost pressures in acute (non-psychiatric) services. Therefore, despite reservations, the payment by results system is probably one that mental health services should join if a viable system can be introduced.
The rationale behind payment by results in the NHS.
The Department of Health believes that payment by results will encourage providers to increase the level of their activity and improve their efficiency. It should provide an incentive for commissioners to seek out lower-cost forms of care in order to reuse the money saved. Payment by results requires an improvement in information systems, which should lead to wider benefits. In addition, services should become more personalised and responsive.
Payment by results in England
A pilot is underway in England to develop clinically meaningful and appropriate classifications (‘currencies’) to accurately describe mental healthcare received by adults of working age and older.
Andrew Fairbairn
Advances in Psychiatric Treatment (2007), vol. 13, 3–6 doi
https://www.cambridge.org/core/journals/advances-in-psychiatric-treatment/article/payment-by-results-in-mental-health-the-current-state-of-play-in-england/AA2E5C377A46E4019604924D28D24522
Abstract
The Department of Health is introducing a 'payment by results' system for mental health services in the UK. The system is already being used in the acute healthcare sector, but is still under development for application in mental healthcare. This article outlines the concept of payment by results, briefly reports on its use in other countries and describes the pilot study underway in England to define currencies to be used in a payment by results system planned for NHS mental healthcare throughout England and Wales.
‘Payment by results’ is a method of paying for the services of hospitals and other providers. Plans are well underway to use it within the National Health Service (NHS) in England, and some health authorities began to introduce it in 2005. The discussion of payment by results is usually peppered with abbreviations. I have used these only rarely in this article, but a list of those most commonly encountered in the literature appears.
Payment by results has three central components.
The first is activity-based funding, which contrasts with the more traditional block contract agreements. For service providers, more work will generate more income or, indeed, less work will generate less.
Second, the amount of work tends to be measured in the context of healthcare resource groups. These are groupings of individual cases that are sufficiently clinically similar and require similar treatment resources. In the acute healthcare sector they tend to be based on international categories of diagnosis. They also take into account procedures, complications and co-existing illnesses. Therefore any payment by results system seeks to provide a coherent manageable way of classifying the mixed cases treated within a hospital. This is why payment by results is sometimes called a system of case-mixed funding.
Third, payment is made according to a national tariff. This tariff is a price tag for any individual healthcare resource group. The price tends to be based on the average cost of treatment across the NHS. This national tariff means that contractual negotiations between commissioners and providers no longer require price negotiation but can concentrate on quantity and quality of care.
It is important to recognise that a number of countries have investigated the possibility of a payment by results system and none so far has successfully implemented such a scheme. Some results of studies in Australia and New Zealand are briefly discussed below but one must draw the conclusion that there maybe a message in this. Nevertheless, the system has been introduced in most of the acute sector of the NHS in England and the Department of Health has put pressure on service commissioners to use it. There is anecdotal evidence that, as the system has not yet been implemented in the mental health sector, commissioners have taken the opportunity to squeeze mental health service funding in order to meet cost pressures in acute (non-psychiatric) services. Therefore, despite reservations, the payment by results system is probably one that mental health services should join if a viable system can be introduced.
The rationale behind payment by results in the NHS.
The Department of Health believes that payment by results will encourage providers to increase the level of their activity and improve their efficiency. It should provide an incentive for commissioners to seek out lower-cost forms of care in order to reuse the money saved. Payment by results requires an improvement in information systems, which should lead to wider benefits. In addition, services should become more personalised and responsive.
Payment by results in England
A pilot is underway in England to develop clinically meaningful and appropriate classifications (‘currencies’) to accurately describe mental healthcare received by adults of working age and older.
Payment by volume (not results) Invited commentary on… Payment by results in mental health
Femi Oyebode
Advances in Psychiatric Treatment (2007), vol. 13, 7–9
Abstract
Payment by results, a system for paying healthcare trusts, is intended as a fair and consistent basis for hospital funding. It relies on a national tariff structured around a case-mix measure known as healthcare resource groups. It is often argued that if payment by results works as planned, the National Health Service will become more efficient and productive. However, the use of a case-mix measure, the healthcare resource group, which derives from the diagnostic related (or diagnosis-related) group, has attendant problems. These include the risk that the payment structure will be inaccurate, unfair and liable to cause the financial destabilisation of trusts. There is also the risk that healthcare institutions will falsify patient classifications (‘up-coding’) to ensure higher remuneration. It has been argued that payment by results may be particularly unsuited to psychiatry. The ability of healthcare resource groups to accurately predict resource use in psychiatry is doubtful. In conclusion, mental health trusts will need to adapt to payment by results but there will inevitably be losers.
Payment by results and diagnosis-related groups
Payment by results is described as a transparent, rules-based system for paying trusts (Department of Health, 2006). It is linked to clinical activity and adjusted for case mix, and is designed to ensure a fair and consistent basis for hospital funding. It replaces commissioning through block agreements and purports to free healthcare funding from historical budgets and the negotiating skills of managers. It relies on a national tariff structured on a casemix measure known as healthcare resource groups. Furthermore, it takes account of regional variation in wages and other costs of service delivery...
As with most things, payment by results is not all that it seems. First, it is best regarded as payment by volume. Its aim is to allow commissioners to commission the volume of activity required to deliver service priorities, from a plurality of providers, on the basis of a standard national price tariff and it is linked to prospective payment and therefore does not rely on results. Central to payment by results is the measure of case mix, the healthcare resource groups (Department of Health, 2006). These are derived from the ‘diagnostic related groups’ that were introduced by legislation in the USA in 1983 as a means of prospective payment for Medicare hospital expenditures.
Diagnosis-related groups are a classification of hospital case types into groups expected to have similar hospital resource use. The groupings are based on diagnoses, age, gender, medical procedures and the presence of complications. Originally, diagnosisrelated groups were expected to have the following attributes: they should be medically meaningful; classes of patients should be grouped together on the basis of variables that are commonly available in hospital discharge summaries; and there should be a manageable number of them. The
characteristics that go into each diagnosis-related group were assumed to have predictive power, i.e. to predict the quantity of hospital resources likely to be consumed on an average hospital stay. In effect, patients are assigned to one of a possible 500 or so diagnosis-related groups and the hospital is prospectively reimbursed a sum.
If the hospital spends less than that sum it achieves a profit that it can keep and if it spends more than that sum, it sustains financial loss. It is easy to see why the expectation is that diagnosis-related groups, like our healthcare resource groups, would drive down cost or, if you wish, would result in greater efficiency.
Benefits and limitations
The real question is how far payment by results is applicable to mental health. Its reliance on healthcare resource groups suggests that there may be problems here. It is acknowledged that the diagnosis-related group system, and by implication healthcare resource groups, faces difficulties in psychiatry and other chronic conditions. My colleagues and I have shown that the term ‘psychoses’, which is one of the top ten diagnosis-related groups and which includes schizophrenia, bipolar affective disorder, psychotic depression and other psychoses, is not homogeneous enough to accurately predict resource utilisation. We found that if length of stay was used as a proxy for resource use, then marital status and electoral ward of residence were better predictors of resource use than diagnosis.
There is little doubt that there is genuine difficulty in applying the diagnosis-related group/healthcare resource group model to psychiatry. It is possible that recognising psychiatric procedures such as rehabilitation, detoxification and intensive in-patient care as classification variables in the same way that surgical procedures are recognised may improve the accuracy of the model. It is also possible that the inclusion of demographic and residential data such as marital status and electoral ward of residence may improve accuracy.
Femi Oyebode
Advances in Psychiatric Treatment (2007), vol. 13, 7–9
Abstract
Payment by results, a system for paying healthcare trusts, is intended as a fair and consistent basis for hospital funding. It relies on a national tariff structured around a case-mix measure known as healthcare resource groups. It is often argued that if payment by results works as planned, the National Health Service will become more efficient and productive. However, the use of a case-mix measure, the healthcare resource group, which derives from the diagnostic related (or diagnosis-related) group, has attendant problems. These include the risk that the payment structure will be inaccurate, unfair and liable to cause the financial destabilisation of trusts. There is also the risk that healthcare institutions will falsify patient classifications (‘up-coding’) to ensure higher remuneration. It has been argued that payment by results may be particularly unsuited to psychiatry. The ability of healthcare resource groups to accurately predict resource use in psychiatry is doubtful. In conclusion, mental health trusts will need to adapt to payment by results but there will inevitably be losers.
Payment by results and diagnosis-related groups
Payment by results is described as a transparent, rules-based system for paying trusts (Department of Health, 2006). It is linked to clinical activity and adjusted for case mix, and is designed to ensure a fair and consistent basis for hospital funding. It replaces commissioning through block agreements and purports to free healthcare funding from historical budgets and the negotiating skills of managers. It relies on a national tariff structured on a casemix measure known as healthcare resource groups. Furthermore, it takes account of regional variation in wages and other costs of service delivery...
As with most things, payment by results is not all that it seems. First, it is best regarded as payment by volume. Its aim is to allow commissioners to commission the volume of activity required to deliver service priorities, from a plurality of providers, on the basis of a standard national price tariff and it is linked to prospective payment and therefore does not rely on results. Central to payment by results is the measure of case mix, the healthcare resource groups (Department of Health, 2006). These are derived from the ‘diagnostic related groups’ that were introduced by legislation in the USA in 1983 as a means of prospective payment for Medicare hospital expenditures.
Diagnosis-related groups are a classification of hospital case types into groups expected to have similar hospital resource use. The groupings are based on diagnoses, age, gender, medical procedures and the presence of complications. Originally, diagnosisrelated groups were expected to have the following attributes: they should be medically meaningful; classes of patients should be grouped together on the basis of variables that are commonly available in hospital discharge summaries; and there should be a manageable number of them. The
characteristics that go into each diagnosis-related group were assumed to have predictive power, i.e. to predict the quantity of hospital resources likely to be consumed on an average hospital stay. In effect, patients are assigned to one of a possible 500 or so diagnosis-related groups and the hospital is prospectively reimbursed a sum.
If the hospital spends less than that sum it achieves a profit that it can keep and if it spends more than that sum, it sustains financial loss. It is easy to see why the expectation is that diagnosis-related groups, like our healthcare resource groups, would drive down cost or, if you wish, would result in greater efficiency.
Benefits and limitations
The real question is how far payment by results is applicable to mental health. Its reliance on healthcare resource groups suggests that there may be problems here. It is acknowledged that the diagnosis-related group system, and by implication healthcare resource groups, faces difficulties in psychiatry and other chronic conditions. My colleagues and I have shown that the term ‘psychoses’, which is one of the top ten diagnosis-related groups and which includes schizophrenia, bipolar affective disorder, psychotic depression and other psychoses, is not homogeneous enough to accurately predict resource utilisation. We found that if length of stay was used as a proxy for resource use, then marital status and electoral ward of residence were better predictors of resource use than diagnosis.
There is little doubt that there is genuine difficulty in applying the diagnosis-related group/healthcare resource group model to psychiatry. It is possible that recognising psychiatric procedures such as rehabilitation, detoxification and intensive in-patient care as classification variables in the same way that surgical procedures are recognised may improve the accuracy of the model. It is also possible that the inclusion of demographic and residential data such as marital status and electoral ward of residence may improve accuracy.
MENTAL HEALTH CARE CLUSTER AND PAYMENT BY RESULTS - CONSIDERATIONS OFR SOCIAL INCLUSION AND RECOVERY
By Michael Clark
Clark, Michael (2011) Mental health care clusters and payment by results: considerations for social inclusion and recovery. Mental Health and Social Inclusion, 15 (2). pp. 71-77. ISSN 2042-8316
DOI: 10.1108/20428301111140912
© 2011 Pier Professional Limited
This version available at: http://eprints.lse.ac.uk/327529/
Available in LSE Research Online: Feb 2012
Abstract:
Recovery and social inclusion ideas and practices have evolved and become widely embedded in mental health care in England over the last decade. These progressive developments need to be nurtured and actively pursued by ensuring that future developments impinging on how mental health care is commissioned and delivered explicitly support them. Payment by Results is being pursued as a policy for commissioning mental health care in England, based on a model of care clusters. These clusters provide some scope for supporting social inclusion and recovery practice, but also some risks. This paper critically examines this emerging policy agenda to identify how we can engage with it to ensure it is supportive of social inclusion and recovery.
It is hoped the improvements towards recovery and social inclusion can continue to flourish in this new world, but we have to be very conscious of the challenges. Progress is more likely if people actively work on emerging policies to build on them to strengthen the cause of inclusion and recovery. We should not underestimate the need to continue to vigorously pursue this agenda, as there are potential risks in the opposite direction from the economic climate and loss of progressive direction during the major system reform of the NHS. As significant continuity throughout this transition between governments has been the national commitment to move to a model of Payment by Results (PbR) in mental health care. This paper discusses the move to PbR and its possible implications for the recovery and social inclusion agenda.
Care clusters and Payment by Results for mental health care:
A consortium of mental health care providers in the North East of England developed a model of care clusters (see Self et al 2008). This model encompasses descriptions of groupings of people needing mental health support based on them having similar needs. The model moves away from purely diagnostic descriptions of people (though not wholly) to one of broadly described needs. There are three super clusters of these groupings, namely non-psychotic (clusters 1-8), psychotic (clusters 10-17) and organic (clusters 18-21).
The mental health care clusters
CARE CLUSTER 1: Common Mental Health Problems (Low Severity)
This group has definite but minor problems of depressed mood, anxiety or other disorder but they do not present with any distressing psychotic symptoms.
CARE CLUSTER 2: Common Mental Health Problems (Low Severity with greater need)
This group has definite but minor problems of depressed mood, anxiety or other disorder but not with any distressing psychotic symptoms. They may have already received care associated with cluster 1 and require more specific intervention or previously been successfully treated at a higher level but are re-presenting with low level symptoms.
CARE CLUSTER 3: Non Psychotic (Moderate Severity)
Moderate problems involving depressed mood, anxiety or other disorder (not including psychosis).
CARE CLUSTER 4: Non-psychotic (Severe)
This group is characterised by severe depression and/or anxiety and/or other increasing complexity of needs. They may experience disruption to function in everyday life and there is an increasing likelihood of significant risks.
CARE CLUSTER 5: Non-psychotic Disorders (Very Severe)
This group will be severely depressed and/or anxious and/or other. They will not present with distressing hallucinations or delusions but may have some unreasonable beliefs. They may often be at high risk for suicide and they may present safeguarding issues and have severe disruption to everyday living.
CARE CLUSTER 6: Non-psychotic Disorder of Over-valued Ideas
Moderate to very severe disorders that are difficult to treat. This may include treatment resistant eating disorder, OCD etc, where extreme beliefs are strongly held, some personality disorders and enduring depression.
CARE CLUSTER 7: Enduring Non-psychotic Disorders (High Disability)
This group suffers from moderate to severe disorders that are very disabling. They will have received treatment for a number of years and although they may have improvement in positive symptoms considerable disability remains that is likely to affect role functioning in many ways.
CARE CLUSTER 8: Non-Psychotic Chaotic and Challenging Disorders
This group will have a wide range of symptoms and chaotic and challenging lifestyles. They are characterised by moderate to very severe repeat deliberate self-harm and/or other impulsive behaviour and chaotic, over dependent engagement and often hostile with services.
CARE CLUSTER 10: First Episode Psychosis
This group will be presenting to the service for the first time with mild to severe psychotic phenomena. They may also have depressed mood and/or anxiety or other behaviours. Drinking or drug-taking may be present but will not be the only problem.
CARE CLUSTER 11: Ongoing Recurrent Psychosis (Low Symptoms)
This group has a history of psychotic symptoms that are currently controlled and causing minor problems if any at all. They are currently experiencing a period of recovery where they are capable of full or near functioning. However, there may be impairment in selfesteem and efficacy and vulnerability to life.
CARE CLUSTER 12: Ongoing or recurrent Psychosis (High Disability)
This group have a history of psychotic symptoms with a significant disability with major impact on role functioning. They are likely to be vulnerable to abuse or exploitation.
CARE CLUSTER 13: Ongoing or Recurrent Psychosis (High Symptom & Disability)
This group will have a history of psychotic symptoms which are not controlled. They will present with severe to very severe psychotic symptoms and some anxiety or depression. They have a significant disability with major impact on role functioning.
CARE CLUSTER 14: Psychotic Crisis
They will be experiencing an acute psychotic episode with severe symptoms that cause severe disruption to role functioning. They may present as vulnerable and a risk to others or themselves.
CARE CLUSTER 15: Severe Psychotic Depression
This group will be suffering from an acute episode of moderate to severe depressive symptoms. Hallucinations and delusions will be present. It is likely that this group will present a risk of suicide and have disruption in many areas of their lives.
CARE CLUSTER 16: Dual Diagnosis
This group has enduring, moderate to severe psychotic or affective symptoms with unstable, chaotic lifestyles and co-existing substance misuse. They may present a risk to self and others and engage poorly with services. Role functioning is often globally impaired.
CARE CLUSTER 17: Psychosis and Affective Disorder – Difficult to Engage
This group has moderate to severe psychotic symptoms with unstable, chaotic lifestyles. There may be some problems with drugs or alcohol not severe enough to warrant dual diagnosis care. This group have a history of non-concordance, are vulnerable & engage poorly with services.
CARE CLUSTER 18: Cognitive Impairment (Low Need)
People who may be in the early stages of dementia (or who may have an organic brain disorder affecting their cognitive function) who have some memory problems, or other low level cognitive impairment but who are still managing to cope reasonably well. Underlying reversible physical causes have been rule out.
CARE CLUSTER 19: Cognitive Impairment or Dementia Complicated (Moderate Need)
People who have problems with their memory, and or other aspects of cognitive functioning resulting in moderate problems looking after themselves and maintaining social relationships. Probable risk of self-neglect or harm to others and may be experiencing some anxiety or depression.
CARE CLUSTER 20: Cognitive Impairment or Dementia Complicated (High Need)
People with dementia who are having significant problems in looking after themselves and whose behaviour may challenge their carers or services. They may have high levels of anxiety or depression, psychotic symptoms or significant problems such as aggression or agitation. The may not be aware of their problems. They are likely to be at high risk of selfneglect or harm to others, and there may be a significant risk of their care arrangements breaking down.
CARE CLUSTER 21: Cognitive Impairment or Dementia (High Physical or Engagement)
People with cognitive impairment or dementia who are having significant problems in looking after themselves, and whose physical condition is becoming increasingly frail. They may not be aware of their problems and there may be a significant risk of their care arrangements breaking down.
CARE CLUSTER 0: Variance
Despite careful consideration of all the other clusters, this group of service users are not adequately described by any of their descriptions. They do however require mental health care and will be offered a service.
Note: In the original version of the clusters model there was a cluster 9, Substance abuse, but this has been removed for now from the Department of Health model for Payment by Results, leaving 9 as a blank.
Allocation to the clusters is based on assessment using the Mental Health Clustering Tool, a framework of items based on the Health of the Nation Outcomes Scale (HoNOS) (Wing et al 1999) with additional questions.
The Mental Health Clustering Tool
Each item is rated by staff on a scale of 0, no problem, to 4, severe to very severe problem.
PART 1: Health of the Nation Outcomes Scale
1. Overactive, aggressive, disruptive or agitated behaviour (current)
2. Non-accidental self-injury (current)
3. Problem-drinking or drug-taking (current)
4. Cognitive problems (current)
5. Physical illness or disability problems (current)
6. Problems associated with hallucinations and delusions (current)
7. Problems with depressed mood (current)
8. Other mental and behavioural problems (current)
9. Problems with relationships (current)
10. Problems with activities of daily living (current)
11. Problems with living conditions (current)
12. Problems with occupation and activities (current)
13. Strong unreasonable beliefs occurring in non-psychotic disorders only. (current) (Additional current question to HoNOS)
PART 2: Historical questions, additional to HoNOS
A. Agitated behaviour/ expansive mood (historical)
B. Repeat self-harm (historical)
C. Safeguarding Children & Vulnerable Dependent Adults (historical)
D. Engagement (historical)
E. Vulnerability (historical)
Source: Department of Health (2010) Mental Health Care Clustering Booklet 2010/11. London: DH
From the care clusters will stem pathways of care for individuals. In principle these will be defined by the individual’s needs and the care cluster the person is deemed to be in. How these clusters and pathways are defined and understood in practice will be significant, then, in how inclusion and recovery are experienced by individuals.
This model of care clusters is being proposed by the Department of Health as the basis for Payment by Results (PbR) in mental health care. PbR is a mode of governance begun under the Labour administrations and continues to be in vogue under the Coalition Government. The presumptions of PbR are that it provides clearer transparency and incentives to service providers to achieve defined goals or results, payment being dependent upon achieving them, and thereby leads to better value for money to commissioners and the tax payer.
Acute hospital care has been moving to PbR with more of their activities being classified by Health Resource Groups (HRGs) (e.g. hip replacements, heart bypass operations etc.). HRGs are the currency for acute PbR, or the things the commissioner purchases. For each unit of currency a tariff (amount of money) is paid. This PbR model in acute care may be characterised as payment by activity as thus far there has been little in the tariff payments dependent on achieving actual results, though the model continues to evolve with more thought given to best practice pathways and defined results as a basis of payments.
For PbR in mental health care the intention is to use the 21 care clusters as the currency, with tariffs to be set for each. Setting a tariff will be challenging given the long term nature of many periods of mental ill health and the diversity of conditions and needs individuals can experience, but it remains the goal of PbR. We should be clear that at this stage only the care cluster model has been defined and widely accepted. There are no accompanying pathways and no tariffs. These will be fundamental to how the system operates and how people experience care.
What are the possible implications for social inclusion and recovery?
With the moves to clusters and pathways, a starting point in considering the issues for social inclusion is to examine the language in the clusters and allocation tool. Care clusters may provide a clarity that eventually enables greater social inclusion, but as a starting point the current language of the care clusters is either ambiguous or unhelpful. Telling someone he or she has a common mental health problem may make him or her feel less stigmatised (like a common cold), or it may feel dismissive at the time of distress. To be openly categorised as ‘non-psychotic chaotic and challenging’ or ‘difficult to engage’ is probably not a helpful opening gambit towards social inclusion.
Similarly the descriptions of the clusters do not help with social inclusion. They are dominated by descriptions of symptoms and problems. The Mental Health Allocation Tool has the potential to draw out some social inclusion issues, such as relationships, activities of daily living, accommodation and occupation. However, these have to be dragged out from under the cover of the process as things seem heavily dominated by risk and symptom issues and a problem oriented starting point, rather than a strengths one. Nor does this process of assessment and allocation start by asking individuals what their recovery goals are.
Of course, the clusters and allocation tool could just be used by clinicians and services as a bureaucratic exercise that has little bearing on changing the ethos of their practice, which could be good or not. The risk and likelihood, however, is that clusters will dramatically influence service ethos and delivery; hence, it would be better if from the beginning they directly and explicitly supported the desired recovery and inclusion orientation.
From a position of wishing to promote recovery and social inclusion then, the language of the clusters model could benefit from a rewrite to make more explicit the issues of recovery and social inclusion. Similarly the allocation tool, which can not easily be rewritten as it is based on HoNOS, at least needs an explicit emphasis placed on a more positive use of the information, leaning towards strengths and social inclusion. We should also begin to make it clearer how these can be made to work within a more recovery and inclusion service ethos and environment.
Looking to what is yet to be developed for the care clusters model, perhaps we can discern a more hopeful position for promoting recovery and social inclusion. Clusters will lead to pathways of care. Pathway is a metaphor to convey an image of a person moving through a service, a journey. This could convey a very narrow understanding of pathways i.e. highly reductionist and directing along a very constrained, common route, with little variation based on individual needs and preferences. If defined in this manner, such pathways might run counter to individual inclusion and recovery.
Pathways could also, however, be defined in a manner that overcomes these negative connotations, and which offers more information and transparency for service users. The model of pathways could also explicitly foreground recovery and social inclusion issues. Pathways could provide consistency of care to ensure people receive what is best and what they are entitled to, including recovery and inclusion based values and practice. Offering a suggested pathway to people provides clarity for initial negotiation and engagement, and a communication device for all parties to be clear on what is expected.
We need to be mindful of how PbR interacts with personalisation, though this will require us to have a critically and sensitively engaged understanding of what personalisation actually means in mental health and social care. Flexibility to offer standard components of care in a more personal way would be a starting point. Further flexibility to tailor addition elements of the care pathway to individual’s needs and preferences, and perhaps their own budgets, would be a further level of personalisation.
How might we build pathways that have clear recovery and social inclusion goals? We need to be clear of the principles, practices and processes of social inclusion that would need to be explicit in pathways. The principles would be to clearly ground the pathways in values and therapeutic aims that are clearly supportive of recovery and social inclusion. Practices would explicitly set out issues and interventions that are relevant to social inclusion. Processes would establish the detail of modes of working, such as care planning, that support recovery and socially inclusive practice.
The good news is that there are articulated recovery and inclusion principles, we have an evidence base for many supportive practices, and we know more about good processes of care, all of which can support recovery and inclusion. The challenge will be of interpretation and codification into exemplar pathways to guide commissioning and practice. It is interesting reading much NICE guidance for mental health, in which the full guidance documents often have statements that would support inclusion and recovery. Yet, discussion of this guidance often defaults to only discussing the detail of specific interventions, such as medication or psychological therapies. This is not to say that the broader values of the NICE guidance are not operationalised in individual clinical settings, but this would be more likely if the pathways could be defined in ways to make inclusion and recovery at the forefront of how care is thought of and delivered. A simple reductionist approach, such as a menu of specific NICE endorsed therapeutic interventions, may run the risk of undermining recovery and inclusion.
Further anchor points to build inclusion and recovery into this model of clusters and PbR are outcomes and quality indicators. Under the proposals of Liberating the NHS, outcomes are to be a fundamental conceptual and organisational principle for health and social care in England. As pointed out by Lawton-Smith (2010), getting these outcomes right for mental health care will be extremely challenging, but profoundly important to what happens to actual delivered care.
Making defined outcomes for the clusters and pathways directly supportive of recovery and inclusion would be a major statement. Tying them to a tariff model is profoundly challenging in principle and in practice, and would need to be cautiously developed and tested, but is a goal we should examine to help the system to evolve to incorporate better support recovery and inclusive practices.
The incentives, disincentives and perverse incentives that a tariff model can contain will need careful attention, and it is here that the current void developing through structural reform of the NHS is challenging, for it is not clear who will be able to direct these issues.
A further risk for social inclusion and recovery from the PbR policy for mental health is that it is presently only directed at the NHS, and not social care. This perennial fault line between health and social care for people experiencing mental health problems could undergo a further fracture through PbR. This is not inevitable, but it is something to be mindful of and to work against. Then there are the other dimensions of inclusion and recovery that need even wider systems working than health and social care, such as accommodation and vocational outcomes. Ensuring that a model of clusters and pathways, and an associated system of PbR, encourages and rewards such broad systems working, rather than fragmenting systems, will be a challenge.
Conclusion:
The multi-faceted and holistic nature of social inclusion and mental health means that no one policy development is the crux for delivering improvements for people. As those who have progressed social inclusion have long since recognised, we need to seek to influence and work with as wide a range of conceptual debates and policy developments as possible. These include work and welfare policies, as well as arts and education, and debates about personalised public services. More recently, we would add the need to engage with debates about the Big Society.
We should be clear, though, that in a sense some policies are more foundational than others, and these are the health and social care policies. If these are not supportive of inclusion and recovery, services experienced by users and their families and carers are less likely to take account of broader inclusion issues.
In emergent approaches and policies like clusters and PbR there will be much that is yet to be defined, and there will be many moving to influence the writing of these missing components in ways that suit their perspectives and interests. Those interested in furthering social inclusion for mental health service users need to engage with these developments to ensure they help individuals and enhance their recovery, inclusion and capabilities in the desired rounded manner.
By Michael Clark
Clark, Michael (2011) Mental health care clusters and payment by results: considerations for social inclusion and recovery. Mental Health and Social Inclusion, 15 (2). pp. 71-77. ISSN 2042-8316
DOI: 10.1108/20428301111140912
© 2011 Pier Professional Limited
This version available at: http://eprints.lse.ac.uk/327529/
Available in LSE Research Online: Feb 2012
Abstract:
Recovery and social inclusion ideas and practices have evolved and become widely embedded in mental health care in England over the last decade. These progressive developments need to be nurtured and actively pursued by ensuring that future developments impinging on how mental health care is commissioned and delivered explicitly support them. Payment by Results is being pursued as a policy for commissioning mental health care in England, based on a model of care clusters. These clusters provide some scope for supporting social inclusion and recovery practice, but also some risks. This paper critically examines this emerging policy agenda to identify how we can engage with it to ensure it is supportive of social inclusion and recovery.
It is hoped the improvements towards recovery and social inclusion can continue to flourish in this new world, but we have to be very conscious of the challenges. Progress is more likely if people actively work on emerging policies to build on them to strengthen the cause of inclusion and recovery. We should not underestimate the need to continue to vigorously pursue this agenda, as there are potential risks in the opposite direction from the economic climate and loss of progressive direction during the major system reform of the NHS. As significant continuity throughout this transition between governments has been the national commitment to move to a model of Payment by Results (PbR) in mental health care. This paper discusses the move to PbR and its possible implications for the recovery and social inclusion agenda.
Care clusters and Payment by Results for mental health care:
A consortium of mental health care providers in the North East of England developed a model of care clusters (see Self et al 2008). This model encompasses descriptions of groupings of people needing mental health support based on them having similar needs. The model moves away from purely diagnostic descriptions of people (though not wholly) to one of broadly described needs. There are three super clusters of these groupings, namely non-psychotic (clusters 1-8), psychotic (clusters 10-17) and organic (clusters 18-21).
The mental health care clusters
CARE CLUSTER 1: Common Mental Health Problems (Low Severity)
This group has definite but minor problems of depressed mood, anxiety or other disorder but they do not present with any distressing psychotic symptoms.
CARE CLUSTER 2: Common Mental Health Problems (Low Severity with greater need)
This group has definite but minor problems of depressed mood, anxiety or other disorder but not with any distressing psychotic symptoms. They may have already received care associated with cluster 1 and require more specific intervention or previously been successfully treated at a higher level but are re-presenting with low level symptoms.
CARE CLUSTER 3: Non Psychotic (Moderate Severity)
Moderate problems involving depressed mood, anxiety or other disorder (not including psychosis).
CARE CLUSTER 4: Non-psychotic (Severe)
This group is characterised by severe depression and/or anxiety and/or other increasing complexity of needs. They may experience disruption to function in everyday life and there is an increasing likelihood of significant risks.
CARE CLUSTER 5: Non-psychotic Disorders (Very Severe)
This group will be severely depressed and/or anxious and/or other. They will not present with distressing hallucinations or delusions but may have some unreasonable beliefs. They may often be at high risk for suicide and they may present safeguarding issues and have severe disruption to everyday living.
CARE CLUSTER 6: Non-psychotic Disorder of Over-valued Ideas
Moderate to very severe disorders that are difficult to treat. This may include treatment resistant eating disorder, OCD etc, where extreme beliefs are strongly held, some personality disorders and enduring depression.
CARE CLUSTER 7: Enduring Non-psychotic Disorders (High Disability)
This group suffers from moderate to severe disorders that are very disabling. They will have received treatment for a number of years and although they may have improvement in positive symptoms considerable disability remains that is likely to affect role functioning in many ways.
CARE CLUSTER 8: Non-Psychotic Chaotic and Challenging Disorders
This group will have a wide range of symptoms and chaotic and challenging lifestyles. They are characterised by moderate to very severe repeat deliberate self-harm and/or other impulsive behaviour and chaotic, over dependent engagement and often hostile with services.
CARE CLUSTER 10: First Episode Psychosis
This group will be presenting to the service for the first time with mild to severe psychotic phenomena. They may also have depressed mood and/or anxiety or other behaviours. Drinking or drug-taking may be present but will not be the only problem.
CARE CLUSTER 11: Ongoing Recurrent Psychosis (Low Symptoms)
This group has a history of psychotic symptoms that are currently controlled and causing minor problems if any at all. They are currently experiencing a period of recovery where they are capable of full or near functioning. However, there may be impairment in selfesteem and efficacy and vulnerability to life.
CARE CLUSTER 12: Ongoing or recurrent Psychosis (High Disability)
This group have a history of psychotic symptoms with a significant disability with major impact on role functioning. They are likely to be vulnerable to abuse or exploitation.
CARE CLUSTER 13: Ongoing or Recurrent Psychosis (High Symptom & Disability)
This group will have a history of psychotic symptoms which are not controlled. They will present with severe to very severe psychotic symptoms and some anxiety or depression. They have a significant disability with major impact on role functioning.
CARE CLUSTER 14: Psychotic Crisis
They will be experiencing an acute psychotic episode with severe symptoms that cause severe disruption to role functioning. They may present as vulnerable and a risk to others or themselves.
CARE CLUSTER 15: Severe Psychotic Depression
This group will be suffering from an acute episode of moderate to severe depressive symptoms. Hallucinations and delusions will be present. It is likely that this group will present a risk of suicide and have disruption in many areas of their lives.
CARE CLUSTER 16: Dual Diagnosis
This group has enduring, moderate to severe psychotic or affective symptoms with unstable, chaotic lifestyles and co-existing substance misuse. They may present a risk to self and others and engage poorly with services. Role functioning is often globally impaired.
CARE CLUSTER 17: Psychosis and Affective Disorder – Difficult to Engage
This group has moderate to severe psychotic symptoms with unstable, chaotic lifestyles. There may be some problems with drugs or alcohol not severe enough to warrant dual diagnosis care. This group have a history of non-concordance, are vulnerable & engage poorly with services.
CARE CLUSTER 18: Cognitive Impairment (Low Need)
People who may be in the early stages of dementia (or who may have an organic brain disorder affecting their cognitive function) who have some memory problems, or other low level cognitive impairment but who are still managing to cope reasonably well. Underlying reversible physical causes have been rule out.
CARE CLUSTER 19: Cognitive Impairment or Dementia Complicated (Moderate Need)
People who have problems with their memory, and or other aspects of cognitive functioning resulting in moderate problems looking after themselves and maintaining social relationships. Probable risk of self-neglect or harm to others and may be experiencing some anxiety or depression.
CARE CLUSTER 20: Cognitive Impairment or Dementia Complicated (High Need)
People with dementia who are having significant problems in looking after themselves and whose behaviour may challenge their carers or services. They may have high levels of anxiety or depression, psychotic symptoms or significant problems such as aggression or agitation. The may not be aware of their problems. They are likely to be at high risk of selfneglect or harm to others, and there may be a significant risk of their care arrangements breaking down.
CARE CLUSTER 21: Cognitive Impairment or Dementia (High Physical or Engagement)
People with cognitive impairment or dementia who are having significant problems in looking after themselves, and whose physical condition is becoming increasingly frail. They may not be aware of their problems and there may be a significant risk of their care arrangements breaking down.
CARE CLUSTER 0: Variance
Despite careful consideration of all the other clusters, this group of service users are not adequately described by any of their descriptions. They do however require mental health care and will be offered a service.
Note: In the original version of the clusters model there was a cluster 9, Substance abuse, but this has been removed for now from the Department of Health model for Payment by Results, leaving 9 as a blank.
Allocation to the clusters is based on assessment using the Mental Health Clustering Tool, a framework of items based on the Health of the Nation Outcomes Scale (HoNOS) (Wing et al 1999) with additional questions.
The Mental Health Clustering Tool
Each item is rated by staff on a scale of 0, no problem, to 4, severe to very severe problem.
PART 1: Health of the Nation Outcomes Scale
1. Overactive, aggressive, disruptive or agitated behaviour (current)
2. Non-accidental self-injury (current)
3. Problem-drinking or drug-taking (current)
4. Cognitive problems (current)
5. Physical illness or disability problems (current)
6. Problems associated with hallucinations and delusions (current)
7. Problems with depressed mood (current)
8. Other mental and behavioural problems (current)
9. Problems with relationships (current)
10. Problems with activities of daily living (current)
11. Problems with living conditions (current)
12. Problems with occupation and activities (current)
13. Strong unreasonable beliefs occurring in non-psychotic disorders only. (current) (Additional current question to HoNOS)
PART 2: Historical questions, additional to HoNOS
A. Agitated behaviour/ expansive mood (historical)
B. Repeat self-harm (historical)
C. Safeguarding Children & Vulnerable Dependent Adults (historical)
D. Engagement (historical)
E. Vulnerability (historical)
Source: Department of Health (2010) Mental Health Care Clustering Booklet 2010/11. London: DH
From the care clusters will stem pathways of care for individuals. In principle these will be defined by the individual’s needs and the care cluster the person is deemed to be in. How these clusters and pathways are defined and understood in practice will be significant, then, in how inclusion and recovery are experienced by individuals.
This model of care clusters is being proposed by the Department of Health as the basis for Payment by Results (PbR) in mental health care. PbR is a mode of governance begun under the Labour administrations and continues to be in vogue under the Coalition Government. The presumptions of PbR are that it provides clearer transparency and incentives to service providers to achieve defined goals or results, payment being dependent upon achieving them, and thereby leads to better value for money to commissioners and the tax payer.
Acute hospital care has been moving to PbR with more of their activities being classified by Health Resource Groups (HRGs) (e.g. hip replacements, heart bypass operations etc.). HRGs are the currency for acute PbR, or the things the commissioner purchases. For each unit of currency a tariff (amount of money) is paid. This PbR model in acute care may be characterised as payment by activity as thus far there has been little in the tariff payments dependent on achieving actual results, though the model continues to evolve with more thought given to best practice pathways and defined results as a basis of payments.
For PbR in mental health care the intention is to use the 21 care clusters as the currency, with tariffs to be set for each. Setting a tariff will be challenging given the long term nature of many periods of mental ill health and the diversity of conditions and needs individuals can experience, but it remains the goal of PbR. We should be clear that at this stage only the care cluster model has been defined and widely accepted. There are no accompanying pathways and no tariffs. These will be fundamental to how the system operates and how people experience care.
What are the possible implications for social inclusion and recovery?
With the moves to clusters and pathways, a starting point in considering the issues for social inclusion is to examine the language in the clusters and allocation tool. Care clusters may provide a clarity that eventually enables greater social inclusion, but as a starting point the current language of the care clusters is either ambiguous or unhelpful. Telling someone he or she has a common mental health problem may make him or her feel less stigmatised (like a common cold), or it may feel dismissive at the time of distress. To be openly categorised as ‘non-psychotic chaotic and challenging’ or ‘difficult to engage’ is probably not a helpful opening gambit towards social inclusion.
Similarly the descriptions of the clusters do not help with social inclusion. They are dominated by descriptions of symptoms and problems. The Mental Health Allocation Tool has the potential to draw out some social inclusion issues, such as relationships, activities of daily living, accommodation and occupation. However, these have to be dragged out from under the cover of the process as things seem heavily dominated by risk and symptom issues and a problem oriented starting point, rather than a strengths one. Nor does this process of assessment and allocation start by asking individuals what their recovery goals are.
Of course, the clusters and allocation tool could just be used by clinicians and services as a bureaucratic exercise that has little bearing on changing the ethos of their practice, which could be good or not. The risk and likelihood, however, is that clusters will dramatically influence service ethos and delivery; hence, it would be better if from the beginning they directly and explicitly supported the desired recovery and inclusion orientation.
From a position of wishing to promote recovery and social inclusion then, the language of the clusters model could benefit from a rewrite to make more explicit the issues of recovery and social inclusion. Similarly the allocation tool, which can not easily be rewritten as it is based on HoNOS, at least needs an explicit emphasis placed on a more positive use of the information, leaning towards strengths and social inclusion. We should also begin to make it clearer how these can be made to work within a more recovery and inclusion service ethos and environment.
Looking to what is yet to be developed for the care clusters model, perhaps we can discern a more hopeful position for promoting recovery and social inclusion. Clusters will lead to pathways of care. Pathway is a metaphor to convey an image of a person moving through a service, a journey. This could convey a very narrow understanding of pathways i.e. highly reductionist and directing along a very constrained, common route, with little variation based on individual needs and preferences. If defined in this manner, such pathways might run counter to individual inclusion and recovery.
Pathways could also, however, be defined in a manner that overcomes these negative connotations, and which offers more information and transparency for service users. The model of pathways could also explicitly foreground recovery and social inclusion issues. Pathways could provide consistency of care to ensure people receive what is best and what they are entitled to, including recovery and inclusion based values and practice. Offering a suggested pathway to people provides clarity for initial negotiation and engagement, and a communication device for all parties to be clear on what is expected.
We need to be mindful of how PbR interacts with personalisation, though this will require us to have a critically and sensitively engaged understanding of what personalisation actually means in mental health and social care. Flexibility to offer standard components of care in a more personal way would be a starting point. Further flexibility to tailor addition elements of the care pathway to individual’s needs and preferences, and perhaps their own budgets, would be a further level of personalisation.
How might we build pathways that have clear recovery and social inclusion goals? We need to be clear of the principles, practices and processes of social inclusion that would need to be explicit in pathways. The principles would be to clearly ground the pathways in values and therapeutic aims that are clearly supportive of recovery and social inclusion. Practices would explicitly set out issues and interventions that are relevant to social inclusion. Processes would establish the detail of modes of working, such as care planning, that support recovery and socially inclusive practice.
The good news is that there are articulated recovery and inclusion principles, we have an evidence base for many supportive practices, and we know more about good processes of care, all of which can support recovery and inclusion. The challenge will be of interpretation and codification into exemplar pathways to guide commissioning and practice. It is interesting reading much NICE guidance for mental health, in which the full guidance documents often have statements that would support inclusion and recovery. Yet, discussion of this guidance often defaults to only discussing the detail of specific interventions, such as medication or psychological therapies. This is not to say that the broader values of the NICE guidance are not operationalised in individual clinical settings, but this would be more likely if the pathways could be defined in ways to make inclusion and recovery at the forefront of how care is thought of and delivered. A simple reductionist approach, such as a menu of specific NICE endorsed therapeutic interventions, may run the risk of undermining recovery and inclusion.
Further anchor points to build inclusion and recovery into this model of clusters and PbR are outcomes and quality indicators. Under the proposals of Liberating the NHS, outcomes are to be a fundamental conceptual and organisational principle for health and social care in England. As pointed out by Lawton-Smith (2010), getting these outcomes right for mental health care will be extremely challenging, but profoundly important to what happens to actual delivered care.
Making defined outcomes for the clusters and pathways directly supportive of recovery and inclusion would be a major statement. Tying them to a tariff model is profoundly challenging in principle and in practice, and would need to be cautiously developed and tested, but is a goal we should examine to help the system to evolve to incorporate better support recovery and inclusive practices.
The incentives, disincentives and perverse incentives that a tariff model can contain will need careful attention, and it is here that the current void developing through structural reform of the NHS is challenging, for it is not clear who will be able to direct these issues.
A further risk for social inclusion and recovery from the PbR policy for mental health is that it is presently only directed at the NHS, and not social care. This perennial fault line between health and social care for people experiencing mental health problems could undergo a further fracture through PbR. This is not inevitable, but it is something to be mindful of and to work against. Then there are the other dimensions of inclusion and recovery that need even wider systems working than health and social care, such as accommodation and vocational outcomes. Ensuring that a model of clusters and pathways, and an associated system of PbR, encourages and rewards such broad systems working, rather than fragmenting systems, will be a challenge.
Conclusion:
The multi-faceted and holistic nature of social inclusion and mental health means that no one policy development is the crux for delivering improvements for people. As those who have progressed social inclusion have long since recognised, we need to seek to influence and work with as wide a range of conceptual debates and policy developments as possible. These include work and welfare policies, as well as arts and education, and debates about personalised public services. More recently, we would add the need to engage with debates about the Big Society.
We should be clear, though, that in a sense some policies are more foundational than others, and these are the health and social care policies. If these are not supportive of inclusion and recovery, services experienced by users and their families and carers are less likely to take account of broader inclusion issues.
In emergent approaches and policies like clusters and PbR there will be much that is yet to be defined, and there will be many moving to influence the writing of these missing components in ways that suit their perspectives and interests. Those interested in furthering social inclusion for mental health service users need to engage with these developments to ensure they help individuals and enhance their recovery, inclusion and capabilities in the desired rounded manner.
Prospective payment systems and discretionary coding—Evidence from English mental health providers
Giuseppe Moscelli, Rowena Jacobs, Nils Gutacker, Maria Jose Aragón, Martin Chalkley, Anne Mason, Jan Böhnke
November 2018
https://onlinelibrary.wiley.com/doi/pdfdirect/10.1002/hec.3851
ABSTRACT
Reimbursement of English mental health hospitals is moving away from block contracts and towards activity and outcome‐based payments. Under the new model, patients are categorised into 20 groups with similar levels of need, called clusters, to which prices may be assigned prospectively. Clinicians, who make clustering decisions, have substantial discretion and can, in principle, directly influence the level of reimbursement the hospital receives. This may create incentives for upcoding. Clinicians are supported in their allocation decision by a clinical clustering algorithm, the Mental Health Clustering Tool, which provides an external reference against which clustering behaviour can be benchmarked. The aims of this study are to investigate the degree of mismatch between predicted and actual clustering and to test whether there are systematic differences amongst providers in their clustering behaviour. We use administrative data for all mental health patients in England who were clustered for the first time during the financial year 2014/15 and estimate multinomial multilevel models of over, under, or matching clustering. Results suggest that hospitals vary systematically in their probability of mismatch but this variation is not consistently associated with observed hospital characteristics.
INTRODUCTION
Most mental health services in England are provided as a part of the publicly funded National Health Service (NHS) and
are free at the point of delivery to patients. These services have primarily been funded through fixed budgets independent
of the actual services delivered (block contracts) agreed between purchasers (commissioners) and providers of care. These arrangements have typically been negotiated on the basis of historical expenditure. From April 2017, mental health (MH) providers were to be remunerated through one of two approaches (NHS England, 2016; NHS Improvement, 2017): (a) a capitation payment model, which is a per‐person risk adjusted sum to cover a range of care for the population across a number of different settings or (b) an episodic payment model, which rewards providers according to the number and type of patients they treat, and sometimes the quality of care they provide, similar to the prospective payment system (PPS) used to fund acute hospital care in England and other countries. In both payment approaches, prices for mental health care (either per patient or per treatment) are set locally.
In this article, we focus on the episodic payment system. In this system, patients are categorised into one of 20 clusters according to need, and these clusters are grouped into one of three superclasses (nonpsychotic, psychotic, organic) depending on the prevalent profile and MH disorder of the patient. Under the episodic payment approach,
each cluster will attract a fixed daily price, which is different for inpatient (admitted) and outpatient (nonadmitted) care.
Clusters also define the relevant period of care, and the system requires patients to be reviewed and assigned to clusters according to those periods. The clusters are mutually exclusive meaning that a patient should only be assigned to one cluster at any given time. Patients are assigned to a cluster by a clinician or clinical team, who can be assisted in their assignment process (known as “clustering”) by an algorithm, called the Mental Health Clustering Tool (MHCT). The paper‐based MHCT, which has been recommended for use since 2013 (Monitor and NHS England, 2013a, 2013b), consists of 18 items and combines information from the 13 items of the Health of the Nation Outcomes Scales, a routine outcome measure used in mental health services, and the five items of the Summary Assessment of Risk and Need (SARN) instrument, which assesses need and risk on both a current and historical basis. A computerised version of the MHCT algorithm has been developed to support clinicians and provides a probability of a patient being assigned to a particular cluster. The MHCT has been designed “to ensure consistency of clustering and to improve the overall accuracy of cluster allocation”. A clinician is, however, able to override the algorithm allocation and the ultimate classification is based on clinical judgement.
The reimbursement of mental health care will be based on the patients' categorisation into clusters. In particular, the
proposed episodic payment approach links a provider's payment to the volume and type of mental health care activity, independently of how much treatment any individual patient receives or how that treatment is delivered and is thus a form of PPS. The potential advantages and risks of PPS have been discussed extensively in the literature. One key risk is the potential of upcoding in which providers assign patients to categories that maximise payment but do not appropriately reflect patients' needs. In mental health services, upcoding is possible because clustering is performed by members of the clinical team rather than by clinical coders. With only 20 clusters, clinical teams may, to varying degrees, be aware of the relative monetary value attached to each. The use of the computerised version of the MHCT is not mandatory, and its suggested cluster allocation can be manually overridden.
Although the allocation of patients to clusters other than that recommended by the MHCT algorithm could represent an appropriate clinical decision, it could also, intentionally or unintentionally, benefit hospitals financially. Some random variation in clustering is expected because care needs varying across patients and not all risk factors are observable or recorded. This has little effect on providers' reimbursement because the expected payment for a
given (latent) patient type is unaffected. Conversely, any systematic coding differences across providers of care would
raise concerns because it potentially results in an inappropriate allocation of financial resources. Systematic differences
may arise because of differences in unmeasured case mix across providers or because providers engage in discretionary
coding to their advantage. Either mechanism calls into question the appropriateness of reimbursing MH providers based
on clusters.
This work is the first to assess whether providers differ systematically in their coding behaviour and whether this is
associated with their observable characteristics, such as the average cost of care.
DISCUSSION AND CONCLUSIONS
The English NHS is moving to a new reimbursement model for mental health care that links payment to activity, thus aligning the payment system in MH to those common in many physical health care systems. Although this change may
help create a fair and sustainable funding system, there are also well-known risks of unintended consequences such as incentives to inappropriately allocate patients higher payment groups.
We have examined the extent to which the categorisation of NHS patients by MH providers is subject to discretion. For this purpose, we investigated differences between patients' first cluster assignments by clinicians and those assign ments suggested by an external standard, the MHCT algorithm. We find MORs ranging from 1.46 to 1.88, which reflects significant unexplained variation between providers in how they allocate patients to clusters over and above observed need factors.
The considerable degree of discretion in the English MH clustering system has important implications for policymakers in the design and operation of the payment system. Clinical judgement may play a larger role in allocation within the MH context than in acute care where diagnostic information and procedures may be more clear-cut and, hence, auditable. Nevertheless, those responsible for the design of the MH payment system will need to find ways to put checks in place to ensure the integrity and fairness of the reimbursement model. The MHCT may offer a starting point, and providers could be required to justify deviations from the proposed cluster allocation if the level of mismatch breaches certain thresholds. This would require continued development and validation of the MHCT algorithm to ensure that it generates consistent groupings of patients with similar needs (Jacobs, 2014).
Giuseppe Moscelli, Rowena Jacobs, Nils Gutacker, Maria Jose Aragón, Martin Chalkley, Anne Mason, Jan Böhnke
November 2018
https://onlinelibrary.wiley.com/doi/pdfdirect/10.1002/hec.3851
ABSTRACT
Reimbursement of English mental health hospitals is moving away from block contracts and towards activity and outcome‐based payments. Under the new model, patients are categorised into 20 groups with similar levels of need, called clusters, to which prices may be assigned prospectively. Clinicians, who make clustering decisions, have substantial discretion and can, in principle, directly influence the level of reimbursement the hospital receives. This may create incentives for upcoding. Clinicians are supported in their allocation decision by a clinical clustering algorithm, the Mental Health Clustering Tool, which provides an external reference against which clustering behaviour can be benchmarked. The aims of this study are to investigate the degree of mismatch between predicted and actual clustering and to test whether there are systematic differences amongst providers in their clustering behaviour. We use administrative data for all mental health patients in England who were clustered for the first time during the financial year 2014/15 and estimate multinomial multilevel models of over, under, or matching clustering. Results suggest that hospitals vary systematically in their probability of mismatch but this variation is not consistently associated with observed hospital characteristics.
INTRODUCTION
Most mental health services in England are provided as a part of the publicly funded National Health Service (NHS) and
are free at the point of delivery to patients. These services have primarily been funded through fixed budgets independent
of the actual services delivered (block contracts) agreed between purchasers (commissioners) and providers of care. These arrangements have typically been negotiated on the basis of historical expenditure. From April 2017, mental health (MH) providers were to be remunerated through one of two approaches (NHS England, 2016; NHS Improvement, 2017): (a) a capitation payment model, which is a per‐person risk adjusted sum to cover a range of care for the population across a number of different settings or (b) an episodic payment model, which rewards providers according to the number and type of patients they treat, and sometimes the quality of care they provide, similar to the prospective payment system (PPS) used to fund acute hospital care in England and other countries. In both payment approaches, prices for mental health care (either per patient or per treatment) are set locally.
In this article, we focus on the episodic payment system. In this system, patients are categorised into one of 20 clusters according to need, and these clusters are grouped into one of three superclasses (nonpsychotic, psychotic, organic) depending on the prevalent profile and MH disorder of the patient. Under the episodic payment approach,
each cluster will attract a fixed daily price, which is different for inpatient (admitted) and outpatient (nonadmitted) care.
Clusters also define the relevant period of care, and the system requires patients to be reviewed and assigned to clusters according to those periods. The clusters are mutually exclusive meaning that a patient should only be assigned to one cluster at any given time. Patients are assigned to a cluster by a clinician or clinical team, who can be assisted in their assignment process (known as “clustering”) by an algorithm, called the Mental Health Clustering Tool (MHCT). The paper‐based MHCT, which has been recommended for use since 2013 (Monitor and NHS England, 2013a, 2013b), consists of 18 items and combines information from the 13 items of the Health of the Nation Outcomes Scales, a routine outcome measure used in mental health services, and the five items of the Summary Assessment of Risk and Need (SARN) instrument, which assesses need and risk on both a current and historical basis. A computerised version of the MHCT algorithm has been developed to support clinicians and provides a probability of a patient being assigned to a particular cluster. The MHCT has been designed “to ensure consistency of clustering and to improve the overall accuracy of cluster allocation”. A clinician is, however, able to override the algorithm allocation and the ultimate classification is based on clinical judgement.
The reimbursement of mental health care will be based on the patients' categorisation into clusters. In particular, the
proposed episodic payment approach links a provider's payment to the volume and type of mental health care activity, independently of how much treatment any individual patient receives or how that treatment is delivered and is thus a form of PPS. The potential advantages and risks of PPS have been discussed extensively in the literature. One key risk is the potential of upcoding in which providers assign patients to categories that maximise payment but do not appropriately reflect patients' needs. In mental health services, upcoding is possible because clustering is performed by members of the clinical team rather than by clinical coders. With only 20 clusters, clinical teams may, to varying degrees, be aware of the relative monetary value attached to each. The use of the computerised version of the MHCT is not mandatory, and its suggested cluster allocation can be manually overridden.
Although the allocation of patients to clusters other than that recommended by the MHCT algorithm could represent an appropriate clinical decision, it could also, intentionally or unintentionally, benefit hospitals financially. Some random variation in clustering is expected because care needs varying across patients and not all risk factors are observable or recorded. This has little effect on providers' reimbursement because the expected payment for a
given (latent) patient type is unaffected. Conversely, any systematic coding differences across providers of care would
raise concerns because it potentially results in an inappropriate allocation of financial resources. Systematic differences
may arise because of differences in unmeasured case mix across providers or because providers engage in discretionary
coding to their advantage. Either mechanism calls into question the appropriateness of reimbursing MH providers based
on clusters.
This work is the first to assess whether providers differ systematically in their coding behaviour and whether this is
associated with their observable characteristics, such as the average cost of care.
DISCUSSION AND CONCLUSIONS
The English NHS is moving to a new reimbursement model for mental health care that links payment to activity, thus aligning the payment system in MH to those common in many physical health care systems. Although this change may
help create a fair and sustainable funding system, there are also well-known risks of unintended consequences such as incentives to inappropriately allocate patients higher payment groups.
We have examined the extent to which the categorisation of NHS patients by MH providers is subject to discretion. For this purpose, we investigated differences between patients' first cluster assignments by clinicians and those assign ments suggested by an external standard, the MHCT algorithm. We find MORs ranging from 1.46 to 1.88, which reflects significant unexplained variation between providers in how they allocate patients to clusters over and above observed need factors.
The considerable degree of discretion in the English MH clustering system has important implications for policymakers in the design and operation of the payment system. Clinical judgement may play a larger role in allocation within the MH context than in acute care where diagnostic information and procedures may be more clear-cut and, hence, auditable. Nevertheless, those responsible for the design of the MH payment system will need to find ways to put checks in place to ensure the integrity and fairness of the reimbursement model. The MHCT may offer a starting point, and providers could be required to justify deviations from the proposed cluster allocation if the level of mismatch breaches certain thresholds. This would require continued development and validation of the MHCT algorithm to ensure that it generates consistent groupings of patients with similar needs (Jacobs, 2014).
Funding of mental health services: Do available data support episodic payment?
Rowena Jacobs, Martin Chalkley, María José Aragón, Jan R. Böhnke, Mike Clark, Valerie Moran, Simon Gilbody
CHE Research Paper 137
Centre for Health Economics, University of York, York, UK
October 2016
https://www.researchgate.net/publication/309013546_Funding_of_Mental_Health_Services_Do_Available_Data_Support_Episodic_Payment
6. Workshop for mental health commissioners
Alongside the empirical analysis, we wanted to obtain feedback on our results by running a one-day workshop for mental health commissioners. Twenty six commissioners attended from various CCGs across the country, as well as Councils and NHS England. Following presentations by the research team of our analytical work, there was a group discussion about the challenges for mental health commissioning arising from the presented analyses, where commissioners at the workshop are in terms of their developments and plans for funding models and contracting for services, and the landscape in terms of moving forward with new funding models. A number of key topics emerged at the workshop.
6.1 Episodic payment or capitated payment?
Recent guidance (Monitor and NHS England, 2016) has suggested that episodic payment models (which most commissioners seemed familiar with and to have done some level of thinking about) or a new approach of capitation (which most of the commissioners had done little to no thinking about) were acceptable alternatives to block contracts.
It was very clear that there is a wide degree of variation between commissioners in terms of their thinking about and confidence in using care clusters and developing their plans for payment models. Some were only now beginning to think about how to move from a block contract model. A few had variations of block contracts, episodic models and embryonic capitation models operating locally; only one group had clear plans for taking the first steps towards a capitation model in the next financial year and evolving it over the next few years.
Having the choice of options has caused much confusion and anxiety amongst some of the commissioners. They were now more uncertain as to what they should be doing and how to do it. Some had clearly felt, following the guidance from Monitor, that they ought to be developing capitation models to be keeping up with the latest thinking, but this felt like a huge step from their current practice with block contracts and/or seemed to be abandoning their work on episodic models before they had had chance to fully learn about this approach to commissioning. Clearer guidance on these matters from a national body would undoubtedly be helpful to many commissioners. This ought to help the commissioners to understand the journey that they are expected to be on, and provide navigational markers to help them on the way.
It was clear that the idea of capitation models of payment in mental health is very new and, hence, there were some quite diverse views as to what conceptually they might be and how to operationalize them. Overall, capitation seems to be seen as a means to integration of services, particularly between physical and mental health services, and, in essence, is a means of pricing a form of grand ‘block contract’ with sophisticated plans for additional metrics of quality and performance. Capitation can include episodic approaches, e.g. capitation for psychosis patients where they are classified into clusters, but the budget for that person is managed by one mental health Trust that pays for his/her acute and primary treatments.
The issue of integration of a person’s care and its relationship to any payment model was worrying for the commissioners in a number of ways. Links across different health providers is one aspect, but then how to encourage better integration with social care and with housing were other challenges. The issue of linking payments to factors that may be beyond the control of mental health care providers, such as housing, was questioned.
Commissioners are keen to explore new ideas, such as accountable care organisations, outcomes-based commissioning, value-based commissioning, and place-based commissioning, but there seemed to be a need for more guidance from central organisations on these concepts and how they might be best operationalised.
Extrapolating from our understanding of the evidence base about forms of payments and issues of data quality, the idea of a capitation model in the forms discussed seems (at best) optimistic as a way forward. We recognise, though, that there is little in the way of robust evidence about the performance of capitation models in the context of mental health care in England chiefly because they are new, although there are some international examples (Monitor and NHS England, 2014).
6.2 Understanding data
Commissioners seemed to welcome the care cluster model. They appeared to be largely working towards using it as a framework to understand and discuss local patterns of care and variations, rather than as a categorical system to use as a threat against providers.
The degree of understanding of MHSDS and its potential links to developing payment models was, though, very varied amongst the commissioners. There may be an urgent need for more development opportunities for some commissioners to progress their thinking and understanding on these issues, if commissioning and payment models are to deliver improvements in mental health care systems. They would seem to want and need more help on how to understand existing data such as MHSDS. They struggle with the expertise and time to turn national data collections into helpful local insights.
It was recognised that there is much to do to improve data quality overall. Some commissioners have worked with their providers to develop incentives for them to improve their data returns. There was a mixed view as to whether this was now the best way forward, with some feeling it was still important to do so but others seeing that a good payment model would provide the incentives for providers to improve data quality. This, though, still leaves the question of whether the analysis can be good enough for the payment model to provide the right incentives.
Some commissioners discussed thinking about using local datasets to plan their commissioning and contracting work. This sometimes felt as if it was without full consideration of the MHSDS national dataset, and the pros and cons of using different datasets. Other instances were where commissioners were developing local data returns to supplement national data, which did not provide the data they needed for their commissioning plans. Some were very keen to use benchmarking within and across service providers to help focus quality improvement work and drive up value in their local systems. It was recognised that there is, though, some way to go to develop the local and national data and analyses to do this. Plus, once again we run in to the problem of a lack of expertise and capacity to achieve these ambitions for using data. There is a need to be clear of the risks of using local data returns in place of national data for developing payment models. There also seemed to be a lack of expertise in being able to use data other than business and process data, such as epidemiological data, which may be needed for models of capitation payments. The challenges involved in linking data to track people across systems of care to develop, manage and refine capitation models also seemed some way from being fully understood and answered in localities.
6.3 Other risks and challenges
There was a tension between wishing to move on quickly with developing payment models to improve care, whilst also wanting robust analysis to inform decisions, which takes time. Obviously, without good analyses to inform decisions there are risks of developing poor payment systems that introduce, for example, perverse incentives or unfair risks for some parties to the contracts.
Risk in the system was another point that was raised. Some participants felt that risk (most likely meaning financial risk), especially to providers, is necessary to provide incentives for change and to improve data collection. However, a tension was also discussed in the need to pay for existing services and even sometimes to make payments to providers to ‘shore them up’, even if services they provided were less than agreed in the quality goals. Data could play a crucial role in managing these issues as it could provide more clarity about the scale and nature of shortcomings and help to incentivise and monitor improvements in provision. It is unclear at this stage to what degree a payment system on its own can assist with this dilemma of supporting existing provision versus investing in new models.
Related to the point around investment in mental health, commissioners called for more clarity and stability with regard to levels of funding for mental health. The commissioners would welcome clear and consistent messages from the centre and practical tools to increase the level of investment in mental health.
There was mixed practice in terms of commissioning from the independent sector. Much seemed to be in the form of ‘spot purchases’. Some had framework or block contracts. It was recognised that contracting from the statutory, independent and third sectors needs to come closer together in terms of approaches being used locally.
Some commissioners face particular geographical challenges with commissioning and developing new models of services and contracts, for example where boundaries between commissioners and providers are not coterminous. Variation in practices arising from several commissioners working with one provider was one example. Some commissioners have worked together where they contract with the same provider.
Commissioners were keen that there were more opportunities such as this workshop to help them and to share experiences and learning. They especially welcomed the time at the workshop to discuss the issues raised with fellow commissioners. They were also keen on further input from academics on how to understand data and analyses.
Some additional, service-focused issues that the commissioners raised were:
7. Discussion and conclusions
This report has explored the proposed episodic payment approach for mental health services whereby clinicians allocate patients into one of 21 clusters on the basis of similar levels of need using the MHCT. For this episodic payment system to effectively work, we have argued that there should not be too much variation in costs either within clusters, or between providers. The MHCT therefore plays a crucial role in that it needs to assign patients to clusters, such that they are homogenous in terms of 1) patient need, and 2) resource use.
We test whether the existing data collected on mental health activity amongst NHS providers within the MHSDS would support this new payment system. Specifically we examine whether there is homogeneity within clusters in terms of 1) costs, and 2) activity/resource use, and 3) whether the MHCT effectively clusters people with similar levels of need.
In this report we have been concerned with examining the relative variation across providers in terms of activity rates and costs. Our results suggest a large amount of variation between providers in terms of costs, activity rates and length of stay within clusters. Our results show that there is substantial variability across providers in the length of cluster episodes, and there is huge variability within clusters in terms of the proportion of inpatient days and the proportion of contact with healthcare professionals. Longer cluster episodes do not translate into proportionally more activity in terms of either inpatient days or contacts with healthcare professionals. With high levels of variation within clusters, accurate baseline activity rates cannot be determined for commissioning.
Variation in activity rates means that providers see different numbers of patients, have different treatment approaches, levels of productivity, and put different care pathways and packages of care in place for patients within each cluster. This could lead to differences in care quality and outcomes across providers, generating potential geographic inequalities for patients. We are unable to say from current data which of these pathways are associated with better outcomes.
At present, there is enormous variation within clusters in terms of costs. Variations in costs mean that patients with similar levels of need may be using different levels of resource, leading to a potential waste of scarce resources. The cost data cannot therefore be used at present to identify a reliable pricing system.
We also found that there is not a great degree of overlap between the MHCT and ‘statistical classes’, generated by sorting patients into classes which are maximally homogeneous within and maximally heterogeneous between. This suggests that there is variation within the 21 clusters created by the MHCT as a classification tool in terms of patient need. The key challenge for the classification system would be to refine the MHCT tool such that it fairly captures similarities and differences between patients. The categories of the classification system need to be casemix homogenous, that is patients within a given care cluster have similar needs profiles.
These key conclusions:
1) significant heterogeneity in patient need,
2) significant heterogeneity in costs, and
3) significant heterogeneity in terms of resource use within clusters,
does not bode very well for an episodic payment approach which requires casemix and resource homogeneity within clusters. The reduction of variations in care, activity levels and costs is therefore pivotal to the establishment of a well-designed classification and payment system. In addition to provider variation, we also observed significant variation between commissioners in terms of their abilities and confidence in developing payment models. Furthermore, we encountered a number of data quality issues in the MHSDS. We found it is not yet able to be used as an information tool to accurately count activity which would be central to its use as a platform for the payment system. There are therefore significant challenges facing the system.
We would argue however, that instead of abandoning the episodic payment approach and clustering altogether, a much clearer steer is needed from policymakers to support providers and commissioners to move towards refining and developing episodic payment as a viable payment option. There is the possibility of re-designing or refining the clusters to improve homogeneity, using the data that has been gathered to date. It has taken more than a decade since implementation in the acute sector to refine and develop the PbR approach. There has been significant investment in information technology and collection of cost data over time which the sector has benefited from. Similar investment in information technology and improvement in data quality needs to be a priority in mental health services. The system also needs to implement change at a pace that does not risk destabilising local health economies. And more research is needed to support evidence-based policy-making and guidance.
We highlight three particular areas of concern and priority:
First, the current policy framework for the funding of mental health care is not providing a clear steer to commissioners and providers of care. Offering the service a choice of payment approach, is causing confusion and anxiety. The current policy proposals offer a lack of clarity, risk further fragmentation, greater local variation and an overall lack of financial control. Providers and commissioners should not be offered a menu of options to payment approaches. This generates further variation at local levels. Once providers and commissioners embark on a particular payment approach, it will be very difficult to change course and re-establish a common set of incentives that can reduce variations. The reality is, that commissioners feel they need to implement the latest ‘trend’ in funding approach, so as not to be left behind. There needs to be a much stronger policy directive on a single best mental health funding approach.
We would argue that the episodic payment approach has several significant advantages over the capitated payment approach and has stronger incentives than the capitated payment approach to increase activity rates and control costs. It may also be simpler to implement, and given capacity constraints within commissioners, may be more pragmatic. The choice of payment approach also has implications for risk attribution between providers and commissioners, with the capitated approach using an Accountable Care Organisation model, shifting risk onto providers. Episodic payment is a more transparent funding approach than the capitated payment approach. Therefore the episodic payment approach has the potential to establish greater parity of esteem between mental and physical health.
The arguments of the ‘institutional bias’ towards acute providers in the funding system is well rehearsed, with larger cuts in tariff prices seen in 2014/15 for mental health services (-1.8%) compared to acute services (-1.5%) (Monitor & NHS England, 2013). Given the current and future projected financial position of providers, with mental health providers delivering overall surpluses year on year, compared to huge increases in deficits year on year for acute providers (Dunn et al, 2016), mental health will continue to be at risk of having their resources diverted away towards acute providers. The disparity in payment systems between mental and physical health care is a major risk factor for mental health services. As long as there are parallel funding systems operating, where in one, better quality activity data and a more transparent system make the return on investment of limited budgets more obvious, it will always win out. Thus as long as mental health operates a block contract system, or an opaque ‘capitation’ contract or variants thereof, commissioners will not have a clear sense of the value for money they are getting from investment in these services and mental health care will lose out.
We would argue that the episodic approach is better developed and has a limited but robust, evidence-base supporting it. The clustering approach is already relatively well established in most providers and could be refined and improved upon. Scrapping it all and starting from scratch risks putting mental health services back almost a decade in terms of developing a more transparent and fair funding system.
With further financial pressures looming, mental health services need a stable funding environment and sustainable commissioning, based on an evidence-informed payment system that generates the right incentives and reduces variations in care.
Second, a fundamental aspect which seems to be missing from the proposed funding models and from discussions with commissioners in any meaningful way, is how any payment system will be linked to quality and outcome metrics. This should be based on sound evidence and not left to local health economies to try to develop. We would argue that it is imperative that the classification and payment system puts incentive structures in place that are able to drive improvements in efficiency of care delivery, without compromising service quality. Again, a stronger policy steer and more evidence is urgently needed and would be found useful.
Third, our research shows that it will be difficult to create a classification and payment system with the currently available data. For the development of any payment system, high quality activity and cost data would be a key requisite. Data quality is a significant challenge with any payment system, but it is at least underway for the episodic payment approach using clustering, collected routinely and we find evidence of some improvements in data quality over time in its collection. We would urge commissioners to routinely use the MHSDS in their contracting and monitoring processes. This is the only way a single consistent use of data can be achieved across several commissioners with any given provider. This prevents providers wasting precious resources filling in different datasets for different commissioners and will incentivise rapid improvement in the data quality of the MHSDS which will facilitate national benchmarking and performance improvement. Commissioners should be offered support to use and understand the MHSDS for local decision-making. Improvements to Reference Cost data are also essential and introduction of Patient Level Information Costing Systems (PLICS) at provider level can support the process of generating this.
In summary: we would call for a clear policy steer to implement and improve the episodic payment approach, underpinned by an imperative to collect high quality activity and cost data that can underpin the classification and payment system. Effort should be put into refining the approach and generating evidence to link appropriate quality and outcome metrics.
Rowena Jacobs, Martin Chalkley, María José Aragón, Jan R. Böhnke, Mike Clark, Valerie Moran, Simon Gilbody
CHE Research Paper 137
Centre for Health Economics, University of York, York, UK
October 2016
https://www.researchgate.net/publication/309013546_Funding_of_Mental_Health_Services_Do_Available_Data_Support_Episodic_Payment
6. Workshop for mental health commissioners
Alongside the empirical analysis, we wanted to obtain feedback on our results by running a one-day workshop for mental health commissioners. Twenty six commissioners attended from various CCGs across the country, as well as Councils and NHS England. Following presentations by the research team of our analytical work, there was a group discussion about the challenges for mental health commissioning arising from the presented analyses, where commissioners at the workshop are in terms of their developments and plans for funding models and contracting for services, and the landscape in terms of moving forward with new funding models. A number of key topics emerged at the workshop.
6.1 Episodic payment or capitated payment?
Recent guidance (Monitor and NHS England, 2016) has suggested that episodic payment models (which most commissioners seemed familiar with and to have done some level of thinking about) or a new approach of capitation (which most of the commissioners had done little to no thinking about) were acceptable alternatives to block contracts.
It was very clear that there is a wide degree of variation between commissioners in terms of their thinking about and confidence in using care clusters and developing their plans for payment models. Some were only now beginning to think about how to move from a block contract model. A few had variations of block contracts, episodic models and embryonic capitation models operating locally; only one group had clear plans for taking the first steps towards a capitation model in the next financial year and evolving it over the next few years.
Having the choice of options has caused much confusion and anxiety amongst some of the commissioners. They were now more uncertain as to what they should be doing and how to do it. Some had clearly felt, following the guidance from Monitor, that they ought to be developing capitation models to be keeping up with the latest thinking, but this felt like a huge step from their current practice with block contracts and/or seemed to be abandoning their work on episodic models before they had had chance to fully learn about this approach to commissioning. Clearer guidance on these matters from a national body would undoubtedly be helpful to many commissioners. This ought to help the commissioners to understand the journey that they are expected to be on, and provide navigational markers to help them on the way.
It was clear that the idea of capitation models of payment in mental health is very new and, hence, there were some quite diverse views as to what conceptually they might be and how to operationalize them. Overall, capitation seems to be seen as a means to integration of services, particularly between physical and mental health services, and, in essence, is a means of pricing a form of grand ‘block contract’ with sophisticated plans for additional metrics of quality and performance. Capitation can include episodic approaches, e.g. capitation for psychosis patients where they are classified into clusters, but the budget for that person is managed by one mental health Trust that pays for his/her acute and primary treatments.
The issue of integration of a person’s care and its relationship to any payment model was worrying for the commissioners in a number of ways. Links across different health providers is one aspect, but then how to encourage better integration with social care and with housing were other challenges. The issue of linking payments to factors that may be beyond the control of mental health care providers, such as housing, was questioned.
Commissioners are keen to explore new ideas, such as accountable care organisations, outcomes-based commissioning, value-based commissioning, and place-based commissioning, but there seemed to be a need for more guidance from central organisations on these concepts and how they might be best operationalised.
Extrapolating from our understanding of the evidence base about forms of payments and issues of data quality, the idea of a capitation model in the forms discussed seems (at best) optimistic as a way forward. We recognise, though, that there is little in the way of robust evidence about the performance of capitation models in the context of mental health care in England chiefly because they are new, although there are some international examples (Monitor and NHS England, 2014).
6.2 Understanding data
Commissioners seemed to welcome the care cluster model. They appeared to be largely working towards using it as a framework to understand and discuss local patterns of care and variations, rather than as a categorical system to use as a threat against providers.
The degree of understanding of MHSDS and its potential links to developing payment models was, though, very varied amongst the commissioners. There may be an urgent need for more development opportunities for some commissioners to progress their thinking and understanding on these issues, if commissioning and payment models are to deliver improvements in mental health care systems. They would seem to want and need more help on how to understand existing data such as MHSDS. They struggle with the expertise and time to turn national data collections into helpful local insights.
It was recognised that there is much to do to improve data quality overall. Some commissioners have worked with their providers to develop incentives for them to improve their data returns. There was a mixed view as to whether this was now the best way forward, with some feeling it was still important to do so but others seeing that a good payment model would provide the incentives for providers to improve data quality. This, though, still leaves the question of whether the analysis can be good enough for the payment model to provide the right incentives.
Some commissioners discussed thinking about using local datasets to plan their commissioning and contracting work. This sometimes felt as if it was without full consideration of the MHSDS national dataset, and the pros and cons of using different datasets. Other instances were where commissioners were developing local data returns to supplement national data, which did not provide the data they needed for their commissioning plans. Some were very keen to use benchmarking within and across service providers to help focus quality improvement work and drive up value in their local systems. It was recognised that there is, though, some way to go to develop the local and national data and analyses to do this. Plus, once again we run in to the problem of a lack of expertise and capacity to achieve these ambitions for using data. There is a need to be clear of the risks of using local data returns in place of national data for developing payment models. There also seemed to be a lack of expertise in being able to use data other than business and process data, such as epidemiological data, which may be needed for models of capitation payments. The challenges involved in linking data to track people across systems of care to develop, manage and refine capitation models also seemed some way from being fully understood and answered in localities.
6.3 Other risks and challenges
There was a tension between wishing to move on quickly with developing payment models to improve care, whilst also wanting robust analysis to inform decisions, which takes time. Obviously, without good analyses to inform decisions there are risks of developing poor payment systems that introduce, for example, perverse incentives or unfair risks for some parties to the contracts.
Risk in the system was another point that was raised. Some participants felt that risk (most likely meaning financial risk), especially to providers, is necessary to provide incentives for change and to improve data collection. However, a tension was also discussed in the need to pay for existing services and even sometimes to make payments to providers to ‘shore them up’, even if services they provided were less than agreed in the quality goals. Data could play a crucial role in managing these issues as it could provide more clarity about the scale and nature of shortcomings and help to incentivise and monitor improvements in provision. It is unclear at this stage to what degree a payment system on its own can assist with this dilemma of supporting existing provision versus investing in new models.
Related to the point around investment in mental health, commissioners called for more clarity and stability with regard to levels of funding for mental health. The commissioners would welcome clear and consistent messages from the centre and practical tools to increase the level of investment in mental health.
There was mixed practice in terms of commissioning from the independent sector. Much seemed to be in the form of ‘spot purchases’. Some had framework or block contracts. It was recognised that contracting from the statutory, independent and third sectors needs to come closer together in terms of approaches being used locally.
Some commissioners face particular geographical challenges with commissioning and developing new models of services and contracts, for example where boundaries between commissioners and providers are not coterminous. Variation in practices arising from several commissioners working with one provider was one example. Some commissioners have worked together where they contract with the same provider.
Commissioners were keen that there were more opportunities such as this workshop to help them and to share experiences and learning. They especially welcomed the time at the workshop to discuss the issues raised with fellow commissioners. They were also keen on further input from academics on how to understand data and analyses.
Some additional, service-focused issues that the commissioners raised were:
- Need for a more coherent approach across the whole system of care, and less firefighting of problems for everyone (e.g. sending patients to A&E in crisis);
- Need to give thought to how to deal with ‘legal highs’.
- Linking of data sets for a more comprehensive analysis, such as HES and MHSDS;
- Analysis of activity and cost per person, especially considering different types of care/modes of delivery (e.g. GP, community mental health, acute mental health, acute physical health).
7. Discussion and conclusions
This report has explored the proposed episodic payment approach for mental health services whereby clinicians allocate patients into one of 21 clusters on the basis of similar levels of need using the MHCT. For this episodic payment system to effectively work, we have argued that there should not be too much variation in costs either within clusters, or between providers. The MHCT therefore plays a crucial role in that it needs to assign patients to clusters, such that they are homogenous in terms of 1) patient need, and 2) resource use.
We test whether the existing data collected on mental health activity amongst NHS providers within the MHSDS would support this new payment system. Specifically we examine whether there is homogeneity within clusters in terms of 1) costs, and 2) activity/resource use, and 3) whether the MHCT effectively clusters people with similar levels of need.
In this report we have been concerned with examining the relative variation across providers in terms of activity rates and costs. Our results suggest a large amount of variation between providers in terms of costs, activity rates and length of stay within clusters. Our results show that there is substantial variability across providers in the length of cluster episodes, and there is huge variability within clusters in terms of the proportion of inpatient days and the proportion of contact with healthcare professionals. Longer cluster episodes do not translate into proportionally more activity in terms of either inpatient days or contacts with healthcare professionals. With high levels of variation within clusters, accurate baseline activity rates cannot be determined for commissioning.
Variation in activity rates means that providers see different numbers of patients, have different treatment approaches, levels of productivity, and put different care pathways and packages of care in place for patients within each cluster. This could lead to differences in care quality and outcomes across providers, generating potential geographic inequalities for patients. We are unable to say from current data which of these pathways are associated with better outcomes.
At present, there is enormous variation within clusters in terms of costs. Variations in costs mean that patients with similar levels of need may be using different levels of resource, leading to a potential waste of scarce resources. The cost data cannot therefore be used at present to identify a reliable pricing system.
We also found that there is not a great degree of overlap between the MHCT and ‘statistical classes’, generated by sorting patients into classes which are maximally homogeneous within and maximally heterogeneous between. This suggests that there is variation within the 21 clusters created by the MHCT as a classification tool in terms of patient need. The key challenge for the classification system would be to refine the MHCT tool such that it fairly captures similarities and differences between patients. The categories of the classification system need to be casemix homogenous, that is patients within a given care cluster have similar needs profiles.
These key conclusions:
1) significant heterogeneity in patient need,
2) significant heterogeneity in costs, and
3) significant heterogeneity in terms of resource use within clusters,
does not bode very well for an episodic payment approach which requires casemix and resource homogeneity within clusters. The reduction of variations in care, activity levels and costs is therefore pivotal to the establishment of a well-designed classification and payment system. In addition to provider variation, we also observed significant variation between commissioners in terms of their abilities and confidence in developing payment models. Furthermore, we encountered a number of data quality issues in the MHSDS. We found it is not yet able to be used as an information tool to accurately count activity which would be central to its use as a platform for the payment system. There are therefore significant challenges facing the system.
We would argue however, that instead of abandoning the episodic payment approach and clustering altogether, a much clearer steer is needed from policymakers to support providers and commissioners to move towards refining and developing episodic payment as a viable payment option. There is the possibility of re-designing or refining the clusters to improve homogeneity, using the data that has been gathered to date. It has taken more than a decade since implementation in the acute sector to refine and develop the PbR approach. There has been significant investment in information technology and collection of cost data over time which the sector has benefited from. Similar investment in information technology and improvement in data quality needs to be a priority in mental health services. The system also needs to implement change at a pace that does not risk destabilising local health economies. And more research is needed to support evidence-based policy-making and guidance.
We highlight three particular areas of concern and priority:
First, the current policy framework for the funding of mental health care is not providing a clear steer to commissioners and providers of care. Offering the service a choice of payment approach, is causing confusion and anxiety. The current policy proposals offer a lack of clarity, risk further fragmentation, greater local variation and an overall lack of financial control. Providers and commissioners should not be offered a menu of options to payment approaches. This generates further variation at local levels. Once providers and commissioners embark on a particular payment approach, it will be very difficult to change course and re-establish a common set of incentives that can reduce variations. The reality is, that commissioners feel they need to implement the latest ‘trend’ in funding approach, so as not to be left behind. There needs to be a much stronger policy directive on a single best mental health funding approach.
We would argue that the episodic payment approach has several significant advantages over the capitated payment approach and has stronger incentives than the capitated payment approach to increase activity rates and control costs. It may also be simpler to implement, and given capacity constraints within commissioners, may be more pragmatic. The choice of payment approach also has implications for risk attribution between providers and commissioners, with the capitated approach using an Accountable Care Organisation model, shifting risk onto providers. Episodic payment is a more transparent funding approach than the capitated payment approach. Therefore the episodic payment approach has the potential to establish greater parity of esteem between mental and physical health.
The arguments of the ‘institutional bias’ towards acute providers in the funding system is well rehearsed, with larger cuts in tariff prices seen in 2014/15 for mental health services (-1.8%) compared to acute services (-1.5%) (Monitor & NHS England, 2013). Given the current and future projected financial position of providers, with mental health providers delivering overall surpluses year on year, compared to huge increases in deficits year on year for acute providers (Dunn et al, 2016), mental health will continue to be at risk of having their resources diverted away towards acute providers. The disparity in payment systems between mental and physical health care is a major risk factor for mental health services. As long as there are parallel funding systems operating, where in one, better quality activity data and a more transparent system make the return on investment of limited budgets more obvious, it will always win out. Thus as long as mental health operates a block contract system, or an opaque ‘capitation’ contract or variants thereof, commissioners will not have a clear sense of the value for money they are getting from investment in these services and mental health care will lose out.
We would argue that the episodic approach is better developed and has a limited but robust, evidence-base supporting it. The clustering approach is already relatively well established in most providers and could be refined and improved upon. Scrapping it all and starting from scratch risks putting mental health services back almost a decade in terms of developing a more transparent and fair funding system.
With further financial pressures looming, mental health services need a stable funding environment and sustainable commissioning, based on an evidence-informed payment system that generates the right incentives and reduces variations in care.
Second, a fundamental aspect which seems to be missing from the proposed funding models and from discussions with commissioners in any meaningful way, is how any payment system will be linked to quality and outcome metrics. This should be based on sound evidence and not left to local health economies to try to develop. We would argue that it is imperative that the classification and payment system puts incentive structures in place that are able to drive improvements in efficiency of care delivery, without compromising service quality. Again, a stronger policy steer and more evidence is urgently needed and would be found useful.
Third, our research shows that it will be difficult to create a classification and payment system with the currently available data. For the development of any payment system, high quality activity and cost data would be a key requisite. Data quality is a significant challenge with any payment system, but it is at least underway for the episodic payment approach using clustering, collected routinely and we find evidence of some improvements in data quality over time in its collection. We would urge commissioners to routinely use the MHSDS in their contracting and monitoring processes. This is the only way a single consistent use of data can be achieved across several commissioners with any given provider. This prevents providers wasting precious resources filling in different datasets for different commissioners and will incentivise rapid improvement in the data quality of the MHSDS which will facilitate national benchmarking and performance improvement. Commissioners should be offered support to use and understand the MHSDS for local decision-making. Improvements to Reference Cost data are also essential and introduction of Patient Level Information Costing Systems (PLICS) at provider level can support the process of generating this.
In summary: we would call for a clear policy steer to implement and improve the episodic payment approach, underpinned by an imperative to collect high quality activity and cost data that can underpin the classification and payment system. Effort should be put into refining the approach and generating evidence to link appropriate quality and outcome metrics.
Making it personal for everyone from block contracts towards individual service funds
Steve Scown and Helen Sanderson, 2021
The future of traditional care services has been the subject of heated debate for longer than Dimensions has been in existence. Enabling people to have a greater say over the services they receive and a role in their delivery is a central theme of the government’s ‘personalisation’ agenda. Dimensions wholeheartedly supports this policy and has been working for a number of years to make it real. However, this agenda does present us with some fundamental challenges we must face up to.
As is the case with many providers, we support large numbers of people who live, and will probably continue to live, in what we describe as a traditional (shared) service (sometimes called residential care homes or group living). While some services provide very good support, there is no escaping the fundamental flaw: the people have not chosen who they live with and, because the team on duty works with everyone, they have a limited choice about who supports them and how their time is spent. Therefore it is perhaps not surprising that few people with a personal budget want to be supported in such a traditional service.
Despite this, we decided, albeit very reluctantly, to face the hard reality that in the current financial climate, closing all of our of traditional homes and helping the people who live in them to acquire their own home and co-design and produce their own support was not going to happen. So what should providers with large numbers of traditional services do? We felt this was the most important challenge Dimensions would face over the coming years.
Steve Scown and Helen Sanderson, 2021
The future of traditional care services has been the subject of heated debate for longer than Dimensions has been in existence. Enabling people to have a greater say over the services they receive and a role in their delivery is a central theme of the government’s ‘personalisation’ agenda. Dimensions wholeheartedly supports this policy and has been working for a number of years to make it real. However, this agenda does present us with some fundamental challenges we must face up to.
As is the case with many providers, we support large numbers of people who live, and will probably continue to live, in what we describe as a traditional (shared) service (sometimes called residential care homes or group living). While some services provide very good support, there is no escaping the fundamental flaw: the people have not chosen who they live with and, because the team on duty works with everyone, they have a limited choice about who supports them and how their time is spent. Therefore it is perhaps not surprising that few people with a personal budget want to be supported in such a traditional service.
Despite this, we decided, albeit very reluctantly, to face the hard reality that in the current financial climate, closing all of our of traditional homes and helping the people who live in them to acquire their own home and co-design and produce their own support was not going to happen. So what should providers with large numbers of traditional services do? We felt this was the most important challenge Dimensions would face over the coming years.
Models for paying providers of NHS services
Block contracts have been widely used throughout the UK, and continue to be the main payment system for hospitals in Scotland, Wales and Northern Ireland.
In England, the national tariff (payment by results) currently dominates payments made to the acute sector.
New, integrated models of care mean that other ways to pay providers may become more dominant.
Block contracts
A block contract is a payment made to a provider to deliver a specific, usually broadly-defined, service. For example, a hospital could be given a block contract to undertake acute care in a particular area.
How the value of a block contract is calculated varies widely. It can be set through a measure of patient need or it may be based on the historical spend of a particular service.
Pros
Capitation
Capitation is a payment system where lump-sum payments are made to care providers based on the number of patients in a target population, to provide some or all of their care needs. The capitation payment is not linked to how much care is provided.
Capitation is used to determine core funding for UK general practice. However, most sustainability and transformation plans in England also aim to move towards an outcome-based capitated budget.
Pros
The national tariffThe national tariff currently dominates payments made to the acute sector in England. HRGs (health resource groups) are used to determine the pricing for health care services.
The national tariff currently dominates payments made to the acute sector in England. HRGs are used to determine the pricing for health care services.
DRGs/HRGs are not used in the NHS in Scotland, Northern Ireland or Wales, where block contracts remain the dominant payment system.
Pros
Payment for performancePayment-for-performance schemes refer to payment arrangements where providers are financially rewarded for achieving high performance or quality. Each scheme rewards providers in a unique way.
In primary care, the QOF (quality and outcomes framework) rewards GP practices for achieving performance indicators.
Scotland is considering new payment arrangements to QOF for GP practices and Wales has agreed reforms going forward.
Quality metrics or indicators can be broken down into three categories:
The BMA's view (British Medical Association)
The BMA does not support the national tariff, payment by results, as the main way for paying acute providers in England.
Instead we would prefer to see a new payment model introduced that encourages closer working between different parts of the health service, around the needs of patients.
Current payment reforms that focus on capitation look, at present, to be the most realistic way of achieving these aims.
Block contracts have been widely used throughout the UK, and continue to be the main payment system for hospitals in Scotland, Wales and Northern Ireland.
In England, the national tariff (payment by results) currently dominates payments made to the acute sector.
New, integrated models of care mean that other ways to pay providers may become more dominant.
Block contracts
A block contract is a payment made to a provider to deliver a specific, usually broadly-defined, service. For example, a hospital could be given a block contract to undertake acute care in a particular area.
How the value of a block contract is calculated varies widely. It can be set through a measure of patient need or it may be based on the historical spend of a particular service.
Pros
- They are timely, predictable and relatively flexible.
- Payments are made on a regular, usually annual, basis.
- Some commissioners and providers favour block contracts because of the low transaction costs.
- Often used where other payment methods would not be financially viable because of low activity levels or budgetary constraints.
- Lack of transparency and accountability after a payment has been made to a provider.
- As block contracts are made in advance of a service being delivered, unexpected pressures such as increased patient demand or cost of care are not taken into account.
- They do not incentivise improved clinical care or efficiency.
Capitation
Capitation is a payment system where lump-sum payments are made to care providers based on the number of patients in a target population, to provide some or all of their care needs. The capitation payment is not linked to how much care is provided.
Capitation is used to determine core funding for UK general practice. However, most sustainability and transformation plans in England also aim to move towards an outcome-based capitated budget.
Pros
- As a capitated payment is not linked to how much care is provided, providers have the flexibility to spend money on services they think will secure the best outcome for the patient.
- The potential for more integrated care and evidence that professionals work more closely together when working under a capitated budget.
- Evaluations of programmes elsewhere show they are more cost-effective than other payment systems.
- Providers are paid regardless of what they deliver - enabling them to provide as little care as possible to minimise costs.
- They do not necessarily take in to account changes in levels of demand, as has been seen in general practice.
- Services delivered by different organisations require significant capabilities on the provider side - eg coordination between primary and secondary care and sophisticated IT to track individual patients' activities.
The national tariffThe national tariff currently dominates payments made to the acute sector in England. HRGs (health resource groups) are used to determine the pricing for health care services.
The national tariff currently dominates payments made to the acute sector in England. HRGs are used to determine the pricing for health care services.
DRGs/HRGs are not used in the NHS in Scotland, Northern Ireland or Wales, where block contracts remain the dominant payment system.
Pros
- As providers are paid according to levels of activity, it encourages them to treat more patients, which can lead to reduced waiting times.
- Increased efficiency and system-wide cost containment - HRG-based payment systems are calculated using average costs and so this encourages those hospitals with above average costs to become more efficient.
- Potential for providers to skimp on quality in order to reduce their costs and maximise profit.
- ‘Cream skimming’ where providers seek out healthier and/or lower-risk patients, or focus on certain conditions or procedures.
- Despite the inclusion of some best practice tariffs and the CQUIN (commissioning for quality and innovation’ framework), the connection between the national tariff and patient outcomes remains poor.
- It does not facilitate a more coordinated approach to health care delivery, across other sectors or parts of the NHS.
Payment for performancePayment-for-performance schemes refer to payment arrangements where providers are financially rewarded for achieving high performance or quality. Each scheme rewards providers in a unique way.
In primary care, the QOF (quality and outcomes framework) rewards GP practices for achieving performance indicators.
Scotland is considering new payment arrangements to QOF for GP practices and Wales has agreed reforms going forward.
Quality metrics or indicators can be broken down into three categories:
- patient outcomes (such as mortality and readmission rates)
- process measures (such as waiting times and screening rates)
- clinical process measures (such as measuring blood pressure).
- There is evidence that payment-for-performance schemes can lead to a clinically-significant reduction in mortality rates.
- Can lead to improvements in quality in terms of process and clinical process measures.
- They are not guaranteed to improve patient outcomes and other quality measures.
- When financial incentives are used to influence performance, leading to a so-called ‘tick box’ culture, those rewards can undermine performance and worsen motivation.
- Can divert attention from other, unrewarded activities.
- Unlikely that they will save money overall.
The BMA's view (British Medical Association)
The BMA does not support the national tariff, payment by results, as the main way for paying acute providers in England.
Instead we would prefer to see a new payment model introduced that encourages closer working between different parts of the health service, around the needs of patients.
Current payment reforms that focus on capitation look, at present, to be the most realistic way of achieving these aims.
New payment approaches for mental health services
Support for commissioners and providers of mental healthcare to shift to new payment approaches.
Introduction to the new payment approachesThe Five Year Forward View (5YFV) sets out objectives to transform the way in which health and care is organised and delivered. These include an increased focus on person-centred and co-ordinated care for patients. Mental health has a crucial role to play in supporting these objectives.
With increasing pressures on mental health services, providers and commissioners must introduce transparent payment approaches that support timely access to NICE-concordant care. This results in better patient outcomes, and can lead to long-term benefits for the local health economy, as patients have a more sustained recovery with fewer readmissions. Commissioners and providers also need to meet the new access and waits standards, as they are introduced.
Payment arrangements need to support the delivery of holistic, integrated and evidence-based care for the biological, psychological and social issues related to people’s mental health, in the least restrictive setting as close to home as possible, and recognise the delivery of the outcomes that matter to those who use services.
Effective use of data, information and evidence are key to achieving these objectives. Providers and commissioners must work collaboratively to ensure that components are in place to allow them to use data and information to improve care. Further, processes should feed back data and information to frontline staff to support care of individuals, and inform continuous improvement in service design.
This data and information will help providers and commissioners to:
Proposed changes to local payment rules covering mental health servicesIn October 2015 Monitor and NHS England launched a consultation setting out 2 payment options for adult and older people mental health services in 2016/17. These are:
These webinars from Monitor and NHS England provide further information on our shared vision for mental health payment development.
Mental health payments: vision and approachesThis first webinar explains the overall vision for mental health payment in the future, and outlines the different payment approaches of capitation, and year of care/episode of treatment.
Mental health payments: implementing the new approachesThis webinar goes into further detail about the 2 payment options, including:
Payment approaches for mental health servicesThese short guides explain and outline the key components of payment approaches for adult and older people mental health services.
Support for commissioners and providers of mental healthcare to shift to new payment approaches.
Introduction to the new payment approachesThe Five Year Forward View (5YFV) sets out objectives to transform the way in which health and care is organised and delivered. These include an increased focus on person-centred and co-ordinated care for patients. Mental health has a crucial role to play in supporting these objectives.
With increasing pressures on mental health services, providers and commissioners must introduce transparent payment approaches that support timely access to NICE-concordant care. This results in better patient outcomes, and can lead to long-term benefits for the local health economy, as patients have a more sustained recovery with fewer readmissions. Commissioners and providers also need to meet the new access and waits standards, as they are introduced.
Payment arrangements need to support the delivery of holistic, integrated and evidence-based care for the biological, psychological and social issues related to people’s mental health, in the least restrictive setting as close to home as possible, and recognise the delivery of the outcomes that matter to those who use services.
Effective use of data, information and evidence are key to achieving these objectives. Providers and commissioners must work collaboratively to ensure that components are in place to allow them to use data and information to improve care. Further, processes should feed back data and information to frontline staff to support care of individuals, and inform continuous improvement in service design.
This data and information will help providers and commissioners to:
- identify the healthcare needs of the local population
- consider service design and resource use to meet those needs in the most efficient and effective way
- provide clarity on accountability for service delivery, quality of care and potential investment needs
- better facilitate and enable constructive, evidence-based discussions between providers and commissioners
- develop robust local prices
- enable continual improvement to care
Proposed changes to local payment rules covering mental health servicesIn October 2015 Monitor and NHS England launched a consultation setting out 2 payment options for adult and older people mental health services in 2016/17. These are:
- an episode of treatment or year-of-care payment approach
- a capitated payment approach
These webinars from Monitor and NHS England provide further information on our shared vision for mental health payment development.
Mental health payments: vision and approachesThis first webinar explains the overall vision for mental health payment in the future, and outlines the different payment approaches of capitation, and year of care/episode of treatment.
Mental health payments: implementing the new approachesThis webinar goes into further detail about the 2 payment options, including:
- how to adopt these approaches
- potential issues
- pros and cons for each approach
Payment approaches for mental health servicesThese short guides explain and outline the key components of payment approaches for adult and older people mental health services.
- Developing a capitated payment approach for mental health (PDF, 410 KB, 9 pages)
- Developing an episodic payment approach for mental health (PDF, 157 KB, 7 pages)
Developing an episodic payment approach for mental health
This short guide explains what an episodic payment approach is, and the steps involved where this approach is being used for mental health services provided in secondary care. This is one of two payment approaches that providers and commissioners should consider developing; the other is a capitated payment approach.
What is an episodic payment approach?
An episodic payment approach is the payment of an agreed price for all the healthcare provided to a patient during an agreed time period – the episode. The price paid depends on the mental health condition a person is being treated for and any co-morbidities they may have.
Clusters
The units of healthcare used for payment are known as currencies. The mental healthcare clusters were mandated as the currencies for much of adult and older people’s mental healthcare in 2012.1 There are 21 mental healthcare clusters (listed in the table below) and these can be grouped into three broad diagnostic categories: psychotic, non-psychotic and organic. The most appropriate cluster is assigned to a person following their assessment using the mental healthcare clustering tool.2 This tool captures the needs of a person with mental ill health and indicates their likely cluster assignment. All providers are contractually obliged to assign the most appropriate cluster to each patient, and submit this categorisation each month as part of the broader Mental Health Dataset Submission requirements.
Payment based on episode or year of care
Each cluster has a defined outer review time for the reassessment of the person with mental ill health, as shown in the table below. The long-term nature of interactions that people with mental ill health typically have with mental healthcare services means reimbursement on a year-of-care basis is appropriate for many of the clusters. Where care is likely to provided on a short-term basis, payment for the outer review period (episode of care) is preferable.
This short guide explains what an episodic payment approach is, and the steps involved where this approach is being used for mental health services provided in secondary care. This is one of two payment approaches that providers and commissioners should consider developing; the other is a capitated payment approach.
What is an episodic payment approach?
An episodic payment approach is the payment of an agreed price for all the healthcare provided to a patient during an agreed time period – the episode. The price paid depends on the mental health condition a person is being treated for and any co-morbidities they may have.
Clusters
The units of healthcare used for payment are known as currencies. The mental healthcare clusters were mandated as the currencies for much of adult and older people’s mental healthcare in 2012.1 There are 21 mental healthcare clusters (listed in the table below) and these can be grouped into three broad diagnostic categories: psychotic, non-psychotic and organic. The most appropriate cluster is assigned to a person following their assessment using the mental healthcare clustering tool.2 This tool captures the needs of a person with mental ill health and indicates their likely cluster assignment. All providers are contractually obliged to assign the most appropriate cluster to each patient, and submit this categorisation each month as part of the broader Mental Health Dataset Submission requirements.
Payment based on episode or year of care
Each cluster has a defined outer review time for the reassessment of the person with mental ill health, as shown in the table below. The long-term nature of interactions that people with mental ill health typically have with mental healthcare services means reimbursement on a year-of-care basis is appropriate for many of the clusters. Where care is likely to provided on a short-term basis, payment for the outer review period (episode of care) is preferable.
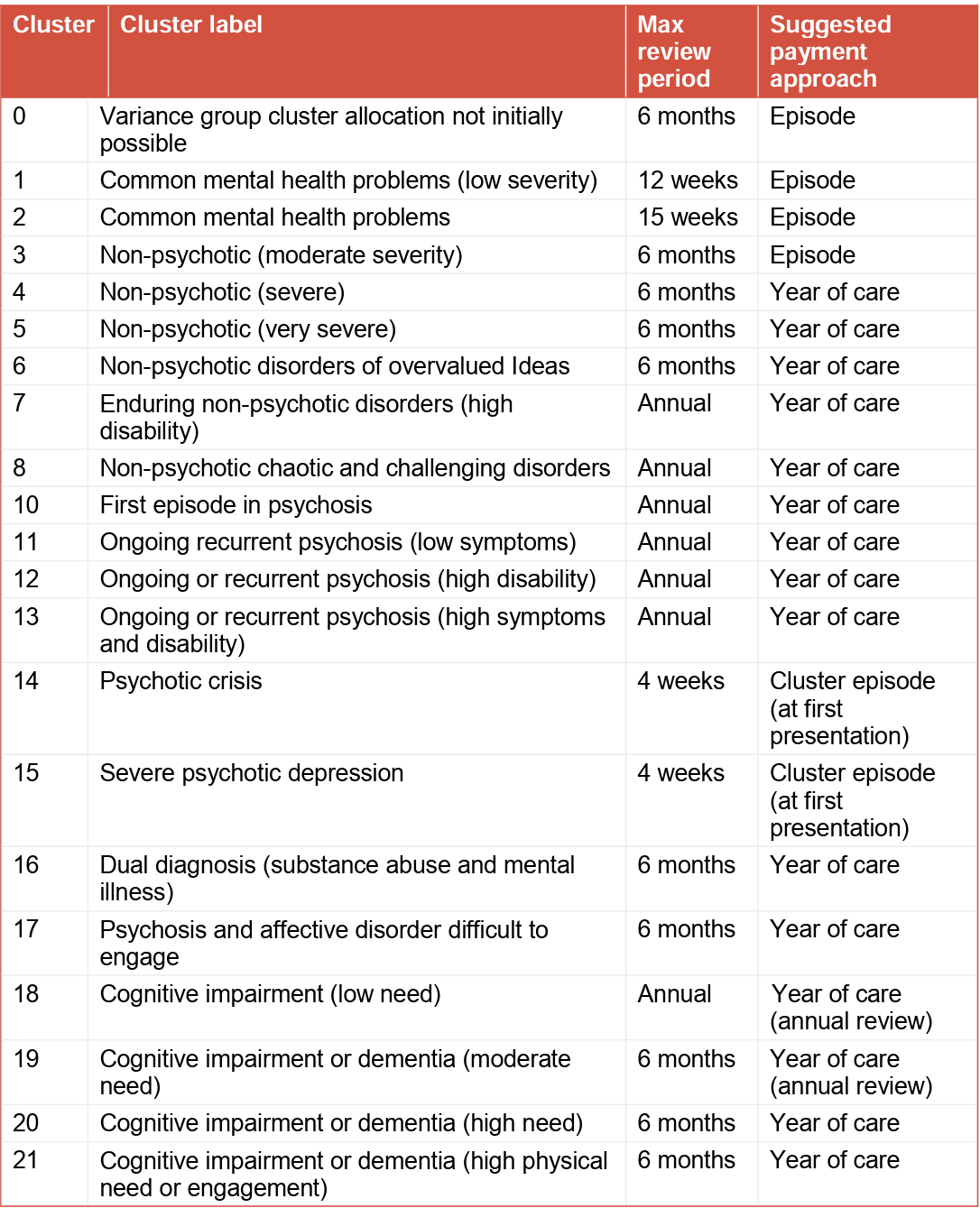
The initial cluster assessment happens when those with mental ill health are first referred to secondary mental healthcare. A provider is paid separately for this assessment, recognising that some people will be assessed as not requiring specialist mental health treatment, or will be referred to other services. These costs are already collected separately in the reference cost collection. The outer review period applies where it has not been possible to assign someone with mental ill health to a cluster (ie those in Cluster 0). The care clusters apply regardless of the setting in which a person with mental ill health is cared for. This means that the agreed price is paid for an episode of care regardless of whether this care is provided in an inpatient setting, in the community or in the home. This approach should provide the right incentives for care to be provided as close to a person’s home as possible, and in the least restrictive setting possible. Clusters 14 and 15 deserve special mention as they represent people experiencing a psychotic crisis. We know from reference cost data that the cost of treating those in psychotic crisis is high. However, we do not want the new payment system to introduce a perverse financial incentive by rewarding providers when patients are in crisis, instead of rewarding them for helping people to manage their condition and avoid crisis. We currently consider a separate payment should be made for up to four weeks of care for anyone in crisis who is accessing mental health services for the first time. Otherwise payment for crisis should form part of the prices agreed for other psychotic clusters. Providers have told us that an increasing number of people experiencing a psychotic crisis as a result of using legal highs are coming into contact with mental health services, sometimes repeatedly. These people do not otherwise have mental health problems but can be very expensive to treat during their crisis. Further, at the end of an inpatient stay they are likely to be referred to drug and alcohol treatment and recovery services or other services not strictly related to mental healthcare. No ICD 10 code captures the use of legal highs, but we consider a separate four-week payment for treating this group to be appropriate.
What are the strengths and limitations of an episodic payment approach?
As with any payment approach there are a number of strengths and weaknesses associated with moving to a new method. Below is an outline of the strengths and limitations of this payment approach. Risk-sharing agreements and caps and collars can be used to manage any financial swings (see below).
Strengths
Greater accountability for and transparency of delivering excellent patient care
Shifts financial risks to commissioners
Requires more active monitoring than a block contract
Limitations
Ensures that money follows the patient so that providers are fully resourced for the care they deliver
Allows the costs of individual patients to be assessed against the outcomes that are being achieved for them, so can assess the value of innovative treatments
What are the necessary components to develop this payment approach? This payment approach makes use of well-established data flows to the Health and Social Care Information Centre (HSCIC). It also builds on what is already being implemented or shadowed in many areas: payment based on mental healthcare cluster currencies. Providers are familiar with submitting reference costs based on the clusters as they have been doing this since 2012, and for the past two years have been required to submit agreed local prices for the care clusters to Monitor. We consider it is essential that outcomes measures become an intrinsic part of the payment mechanism for mental health services. The mental health dataset already contains a number of items that can be used to look at outcomes by cluster. Quality and outcomes measures will need to be agreed and monitored as part of the contract, along with agreement on data reporting and quality assurance of the data. This should include both nationally and locally determined measures. How is this payment approach developed locally? If payment is to be based on an episode of care, both commissioners and providers must have confidence in the internal processes for capturing the data that flow to the HSCIC and the quality of those data. Good quality local data will be needed for the delivery of effective evidence-based services that reflect the needs of local populations. Risk-sharing agreements and caps and collars can help to manage the impacts of a change in the payment approach, particularly in the short term. Such arrangements can also allow providers and commissioners to share financial risks and benefits that may come from different ways of delivering care. A good starting point is to look at current contact values and the active caseload. However, both commissioners and providers need to be mindful of the need to provide care that is effective. Care models must reflect evidence-based approaches to care and National Institute for Health and Care Excellence (NICE) guidance. They must also meet the new access and waits standards to be introduced over the 4 coming year. Meeting these standards may involve additional costs and these need to be factored in when developing local prices. Appropriate attention needs to be given to prevention and early intervention to ensure improved outcomes for those with mental ill health, and the most efficient and effective use of resources. This may require analysis and some bottom-up costing to understand the needs of the population, what the most effective and efficient service design is, and how payment should be developed. The active caseload is the number of people with mental ill health by cluster who are receiving treatment or being assessed. To assess this, data must be cleansed so that only those currently being assessed or receiving treatment are included. The number of people with mental ill health on the current active caseload can be determined by taking a snapshot of caseload analysed by cluster and initial assessment at a particular point in time, or by taking an average over a period. Either way, it is important that active caseload accurately reflects activity and that the process used to determine it is agreed between commissioners and providers. The monthly reports provided by the HSCIC include information on caseload. Where caseload changes are anticipated in the coming years (whether from planned changes to service delivery or demographic changes), they should be agreed by commissioners and providers. They should also be monitored on a quarterly basis, broken down by initial assessment, cluster allocation and treatment. The resources required to provide care to people with mental ill health in each cluster, as well as to conduct their initial assessments, will differ. These differences can be captured by calculating the relative resource intensity (RRI) for each cluster. Although packages of care will be personalised for each person in any single cluster, on average they will use similar levels of resources. The RRI weighting can be used to calculate prices, based on the existing contract value, which reflect the different resource requirements of delivering care to patients assigned to a particular cluster. Organisations that have a patient-level information and costing system (PLICS) can use this system to calculate the RRI. For organisations without such a system, per diem reference costs can be used as a proxy for RRI in the interim. Detailed guidance on calculating the RRI will be published early in 2016.3
Risk sharing
We recognise that moving to any new payment approach has associated risks. These need to be managed to prevent destabilisation of either the providers or commissioners. There are two approaches that could be used:
1. The simplest approach is to set a range for activity changes that have no associated resource implication for commissioners or providers – known as a collar. Activity changes within this range are absorbed in year, but can be reflected by agreement in future years’ contracts. The threshold at which activity triggers payment is locally agreed by providers and commissioners. It is suggested that a level of at least ±5% is set in the first year to reflect the developmental nature of this approach and the continuing underlying issues of data quality. Ideally, such arrangements should be employed at cluster level, but local arrangements may determine that these are aggregated at a total contract level. Any activity changes beyond this threshold will attract funding at 100% of the cluster price.
2. The second approach is to agree a level of variation within which the activity attracts funding adjustments, but outside of which is capped – known as a cap. It is suggested that a low cap level is set (eg ±2%). There will be some volatility as cluster-based contracts are embedded and as a result some variation in activity is driven by data quality rather than demand. This variation needs to be addressed by providers and commissioners, and recorded in either Schedule 3A (Local prices) or in Schedule 2G (Other local agreements, policies and procedures) in the contract. For more information, please refer to the NHS standard contract 2016/17 technical guidance s44.3.4
We strongly recommend that organisations have a memorandum of understanding in place to manage the financial risk for both parties and that this covers:
management of data quality, and arrangements for cleansing caseload activity through the year. This will ensure that changes in caseload arising from data quality improvement rather than changes in demand have no financial implications
arrangements for reflecting service improvement/transformation in the contract
arrangements for re-basing the contract through the year where this is appropriate.
Cluster pathway payment and choice of provider
People with mental ill health have a right to choose a provider for their first outpatient appointment with any clinically appropriate healthcare professional.5 Payment for mental health services which is made on the basis of an episode of care should facilitate choice. We will publish support materials to help commissioners effectively support choice for mental healthcare.
Defining quality and outcomes incentives
In any capitated payment approach providers and commissioners must identify and link payment to quality and outcomes metrics, which will influence the final payment made to the provider(s). This can ensure providers do not sacrifice quality and patient outcomes to generate financial savings. Providers and commissioners must identify the quality and outcomes measures to link to payment. These should include the national measures for mental healthcare that are being developed, but locally determined measures will also be needed. Local measures should be co-developed with all important local stakeholders, ie service users, clinicians, providers and commissioners, and reflect evidence-based approaches to care and NICE guidance. Monitor and NHS England will provide further guidance on using and developing quality and outcomes measures, and how these can be linked to payment.
© Monitor (December 2015) Publication code: IRG 43/15
NHS England Publications Gateway Reference 04464
NHS England Document Classification: Official
What are the strengths and limitations of an episodic payment approach?
As with any payment approach there are a number of strengths and weaknesses associated with moving to a new method. Below is an outline of the strengths and limitations of this payment approach. Risk-sharing agreements and caps and collars can be used to manage any financial swings (see below).
Strengths
Greater accountability for and transparency of delivering excellent patient care
Shifts financial risks to commissioners
Requires more active monitoring than a block contract
Limitations
Ensures that money follows the patient so that providers are fully resourced for the care they deliver
Allows the costs of individual patients to be assessed against the outcomes that are being achieved for them, so can assess the value of innovative treatments
What are the necessary components to develop this payment approach? This payment approach makes use of well-established data flows to the Health and Social Care Information Centre (HSCIC). It also builds on what is already being implemented or shadowed in many areas: payment based on mental healthcare cluster currencies. Providers are familiar with submitting reference costs based on the clusters as they have been doing this since 2012, and for the past two years have been required to submit agreed local prices for the care clusters to Monitor. We consider it is essential that outcomes measures become an intrinsic part of the payment mechanism for mental health services. The mental health dataset already contains a number of items that can be used to look at outcomes by cluster. Quality and outcomes measures will need to be agreed and monitored as part of the contract, along with agreement on data reporting and quality assurance of the data. This should include both nationally and locally determined measures. How is this payment approach developed locally? If payment is to be based on an episode of care, both commissioners and providers must have confidence in the internal processes for capturing the data that flow to the HSCIC and the quality of those data. Good quality local data will be needed for the delivery of effective evidence-based services that reflect the needs of local populations. Risk-sharing agreements and caps and collars can help to manage the impacts of a change in the payment approach, particularly in the short term. Such arrangements can also allow providers and commissioners to share financial risks and benefits that may come from different ways of delivering care. A good starting point is to look at current contact values and the active caseload. However, both commissioners and providers need to be mindful of the need to provide care that is effective. Care models must reflect evidence-based approaches to care and National Institute for Health and Care Excellence (NICE) guidance. They must also meet the new access and waits standards to be introduced over the 4 coming year. Meeting these standards may involve additional costs and these need to be factored in when developing local prices. Appropriate attention needs to be given to prevention and early intervention to ensure improved outcomes for those with mental ill health, and the most efficient and effective use of resources. This may require analysis and some bottom-up costing to understand the needs of the population, what the most effective and efficient service design is, and how payment should be developed. The active caseload is the number of people with mental ill health by cluster who are receiving treatment or being assessed. To assess this, data must be cleansed so that only those currently being assessed or receiving treatment are included. The number of people with mental ill health on the current active caseload can be determined by taking a snapshot of caseload analysed by cluster and initial assessment at a particular point in time, or by taking an average over a period. Either way, it is important that active caseload accurately reflects activity and that the process used to determine it is agreed between commissioners and providers. The monthly reports provided by the HSCIC include information on caseload. Where caseload changes are anticipated in the coming years (whether from planned changes to service delivery or demographic changes), they should be agreed by commissioners and providers. They should also be monitored on a quarterly basis, broken down by initial assessment, cluster allocation and treatment. The resources required to provide care to people with mental ill health in each cluster, as well as to conduct their initial assessments, will differ. These differences can be captured by calculating the relative resource intensity (RRI) for each cluster. Although packages of care will be personalised for each person in any single cluster, on average they will use similar levels of resources. The RRI weighting can be used to calculate prices, based on the existing contract value, which reflect the different resource requirements of delivering care to patients assigned to a particular cluster. Organisations that have a patient-level information and costing system (PLICS) can use this system to calculate the RRI. For organisations without such a system, per diem reference costs can be used as a proxy for RRI in the interim. Detailed guidance on calculating the RRI will be published early in 2016.3
Risk sharing
We recognise that moving to any new payment approach has associated risks. These need to be managed to prevent destabilisation of either the providers or commissioners. There are two approaches that could be used:
1. The simplest approach is to set a range for activity changes that have no associated resource implication for commissioners or providers – known as a collar. Activity changes within this range are absorbed in year, but can be reflected by agreement in future years’ contracts. The threshold at which activity triggers payment is locally agreed by providers and commissioners. It is suggested that a level of at least ±5% is set in the first year to reflect the developmental nature of this approach and the continuing underlying issues of data quality. Ideally, such arrangements should be employed at cluster level, but local arrangements may determine that these are aggregated at a total contract level. Any activity changes beyond this threshold will attract funding at 100% of the cluster price.
2. The second approach is to agree a level of variation within which the activity attracts funding adjustments, but outside of which is capped – known as a cap. It is suggested that a low cap level is set (eg ±2%). There will be some volatility as cluster-based contracts are embedded and as a result some variation in activity is driven by data quality rather than demand. This variation needs to be addressed by providers and commissioners, and recorded in either Schedule 3A (Local prices) or in Schedule 2G (Other local agreements, policies and procedures) in the contract. For more information, please refer to the NHS standard contract 2016/17 technical guidance s44.3.4
We strongly recommend that organisations have a memorandum of understanding in place to manage the financial risk for both parties and that this covers:
management of data quality, and arrangements for cleansing caseload activity through the year. This will ensure that changes in caseload arising from data quality improvement rather than changes in demand have no financial implications
arrangements for reflecting service improvement/transformation in the contract
arrangements for re-basing the contract through the year where this is appropriate.
Cluster pathway payment and choice of provider
People with mental ill health have a right to choose a provider for their first outpatient appointment with any clinically appropriate healthcare professional.5 Payment for mental health services which is made on the basis of an episode of care should facilitate choice. We will publish support materials to help commissioners effectively support choice for mental healthcare.
Defining quality and outcomes incentives
In any capitated payment approach providers and commissioners must identify and link payment to quality and outcomes metrics, which will influence the final payment made to the provider(s). This can ensure providers do not sacrifice quality and patient outcomes to generate financial savings. Providers and commissioners must identify the quality and outcomes measures to link to payment. These should include the national measures for mental healthcare that are being developed, but locally determined measures will also be needed. Local measures should be co-developed with all important local stakeholders, ie service users, clinicians, providers and commissioners, and reflect evidence-based approaches to care and NICE guidance. Monitor and NHS England will provide further guidance on using and developing quality and outcomes measures, and how these can be linked to payment.
© Monitor (December 2015) Publication code: IRG 43/15
NHS England Publications Gateway Reference 04464
NHS England Document Classification: Official
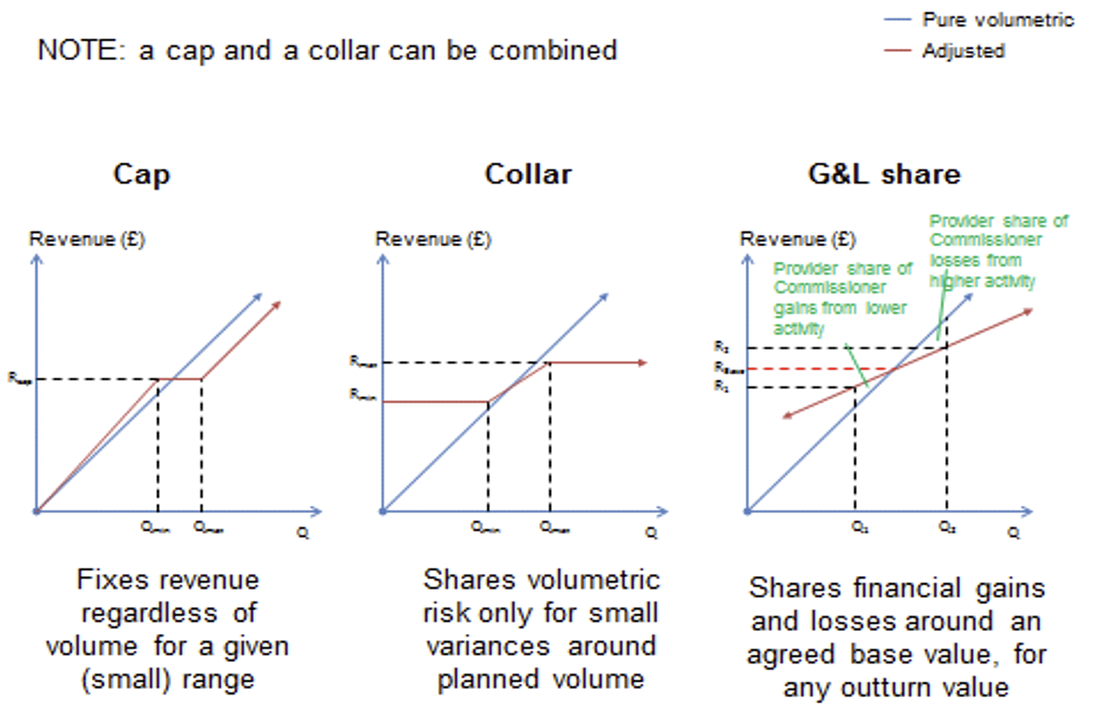
An agreement should also be reached on how any financial gains or losses will be managed and shared. Examples are given in the figure below.
Developing a capitated payment approach for mental health
This short guide explains what a capitated payment approach is, and the steps that need to be taken to adopt this approach for mental health services provided in secondary care. This is one of two payment approaches that providers and commissioners should consider developing; the other is an episodic payment approach. The Five Year Forward View (5YFV) has set out objectives to transform the way healthcare is organised and delivered. Locally developed capitated payment for mental health could support these objectives. To support the development of local payment approaches for mental healthcare, this short guide sets out: what a capitated payment is the models of integrated care that can be supported by capitation the strengths and limitations of capitation the key enablers to developing this payment approach the seven design steps for implementation. Our focus in this guide is how capitated payment can be developed for mental healthcare covered by the mental healthcare clusters (secondary mental healthcare for adults and older people), with some elements of physical, social and community care included. However, the same seven design steps can be used to cover mental healthcare that goes beyond the care clusters (eg children’s and young people’s or secure and forensic mental healthcare). This more limited scope for capitation focused largely on mental healthcare could be a stepping stone to developing fully integrated care models, such as multispecialty community providers (MCPs) or primary and acute care systems (PACS).
What is a capitated payment approach?
A capitated payment approach is the payment of a provider or group of providers to cover a range of care for a population across a number of different care settings. Payments are made on a per person basis and are risk adjusted to reflect the different needs of people with mental ill health. Any capitated payment for mental health must include a component linked to achieving agreed quality and outcome measures. This ensures that providers remain directly accountable for providing timely care that is in the best interest of people with mental ill health. We know that local health economies (LHEs) are looking at new care models that can support their population’s needs more effectively. Capitation can support different models of care, as outlined in the 5YFV, including a ‘fully integrated care model’ and ‘integrated mental health care models’. Payment should then be locally developed to support this. The diagram below shows potential combinations of care models1 and payment approaches.
This short guide explains what a capitated payment approach is, and the steps that need to be taken to adopt this approach for mental health services provided in secondary care. This is one of two payment approaches that providers and commissioners should consider developing; the other is an episodic payment approach. The Five Year Forward View (5YFV) has set out objectives to transform the way healthcare is organised and delivered. Locally developed capitated payment for mental health could support these objectives. To support the development of local payment approaches for mental healthcare, this short guide sets out: what a capitated payment is the models of integrated care that can be supported by capitation the strengths and limitations of capitation the key enablers to developing this payment approach the seven design steps for implementation. Our focus in this guide is how capitated payment can be developed for mental healthcare covered by the mental healthcare clusters (secondary mental healthcare for adults and older people), with some elements of physical, social and community care included. However, the same seven design steps can be used to cover mental healthcare that goes beyond the care clusters (eg children’s and young people’s or secure and forensic mental healthcare). This more limited scope for capitation focused largely on mental healthcare could be a stepping stone to developing fully integrated care models, such as multispecialty community providers (MCPs) or primary and acute care systems (PACS).
What is a capitated payment approach?
A capitated payment approach is the payment of a provider or group of providers to cover a range of care for a population across a number of different care settings. Payments are made on a per person basis and are risk adjusted to reflect the different needs of people with mental ill health. Any capitated payment for mental health must include a component linked to achieving agreed quality and outcome measures. This ensures that providers remain directly accountable for providing timely care that is in the best interest of people with mental ill health. We know that local health economies (LHEs) are looking at new care models that can support their population’s needs more effectively. Capitation can support different models of care, as outlined in the 5YFV, including a ‘fully integrated care model’ and ‘integrated mental health care models’. Payment should then be locally developed to support this. The diagram below shows potential combinations of care models1 and payment approaches.
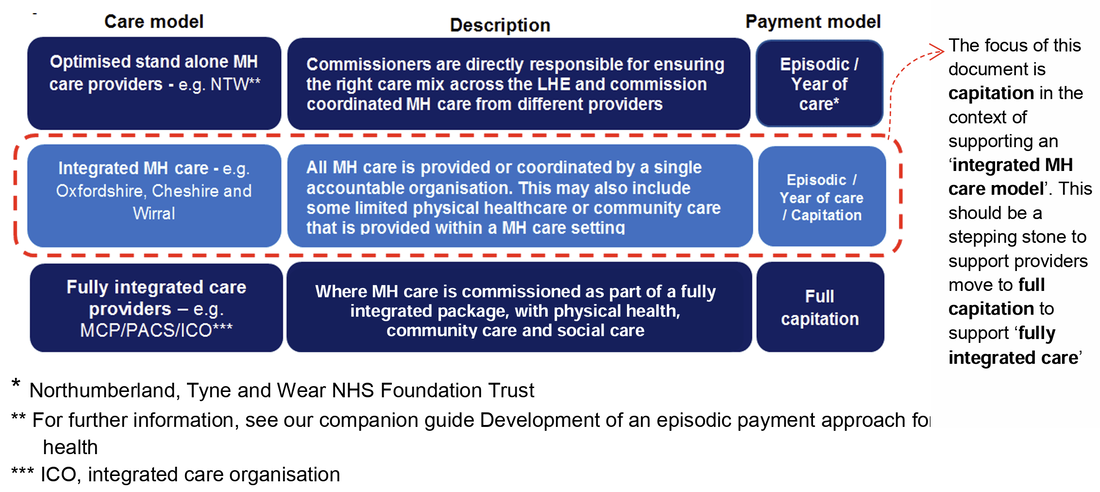
What are the strengths and limitations of a capitated payment approach?
The table below outlines some of the main strengths and limitations of using a capitated payment approach.
Strengths
Strong incentives to invest in early intervention and prevention to avoid potential complications resulting in higher costs
Providers may ‘cherry pick’ patients and restrict access to care if mechanisms are not in place to ensure quality and access
Allows more flexible and efficient allocation of resources for improved efficiency gains
Limitations
Greater accountability for delivering high quality patient care
Risk of cost shifting if service and population scope is not clearly defined
Requires good data on activity, costs and outcomes linked at patient level across relevant providers
Risk of driving down quality of care for financial gains if appropriate mechanisms are not in place
Providers and commissioners should work together to develop and implement local mitigations to the potential risks identified above. Clear governance structures, payment linked to locally developed quality and outcome metrics,3 and the financial gain/loss sharing mechanism4 can help mitigate some of these risks. Also, under a capitated payment arrangement it would be important to ensure patient choice is supported. Where patients’ right to choice applies to a mental health service, commissioners must commission the service from any provider that meets their criteria for providing that service.
The arrangement does not need to be limited to one provider for each type of service; it could, for example, include multiple community providers and/or acute providers. However, including some but not other providers in the arrangement must not restrict patient choice: a patient must not be denied the choice (where applicable) to be referred to a provider that is not part of the arrangement.5 Further, capitation should not prevent patients from having a personal budget, where applicable. People with mental ill health with a personal budget would still enjoy the same choice of services and providers delivering them: the personal budget would be deducted from the total capitation payment and paid instead to the providers chosen by the patients.
What are the enablers to developing a capitated payment approach for mental health?
A number of local enablers are fundamental to the development and implementation of any capitated payment approach for mental health, as shown below.
The table below outlines some of the main strengths and limitations of using a capitated payment approach.
Strengths
Strong incentives to invest in early intervention and prevention to avoid potential complications resulting in higher costs
Providers may ‘cherry pick’ patients and restrict access to care if mechanisms are not in place to ensure quality and access
Allows more flexible and efficient allocation of resources for improved efficiency gains
Limitations
Greater accountability for delivering high quality patient care
Risk of cost shifting if service and population scope is not clearly defined
Requires good data on activity, costs and outcomes linked at patient level across relevant providers
Risk of driving down quality of care for financial gains if appropriate mechanisms are not in place
Providers and commissioners should work together to develop and implement local mitigations to the potential risks identified above. Clear governance structures, payment linked to locally developed quality and outcome metrics,3 and the financial gain/loss sharing mechanism4 can help mitigate some of these risks. Also, under a capitated payment arrangement it would be important to ensure patient choice is supported. Where patients’ right to choice applies to a mental health service, commissioners must commission the service from any provider that meets their criteria for providing that service.
The arrangement does not need to be limited to one provider for each type of service; it could, for example, include multiple community providers and/or acute providers. However, including some but not other providers in the arrangement must not restrict patient choice: a patient must not be denied the choice (where applicable) to be referred to a provider that is not part of the arrangement.5 Further, capitation should not prevent patients from having a personal budget, where applicable. People with mental ill health with a personal budget would still enjoy the same choice of services and providers delivering them: the personal budget would be deducted from the total capitation payment and paid instead to the providers chosen by the patients.
What are the enablers to developing a capitated payment approach for mental health?
A number of local enablers are fundamental to the development and implementation of any capitated payment approach for mental health, as shown below.
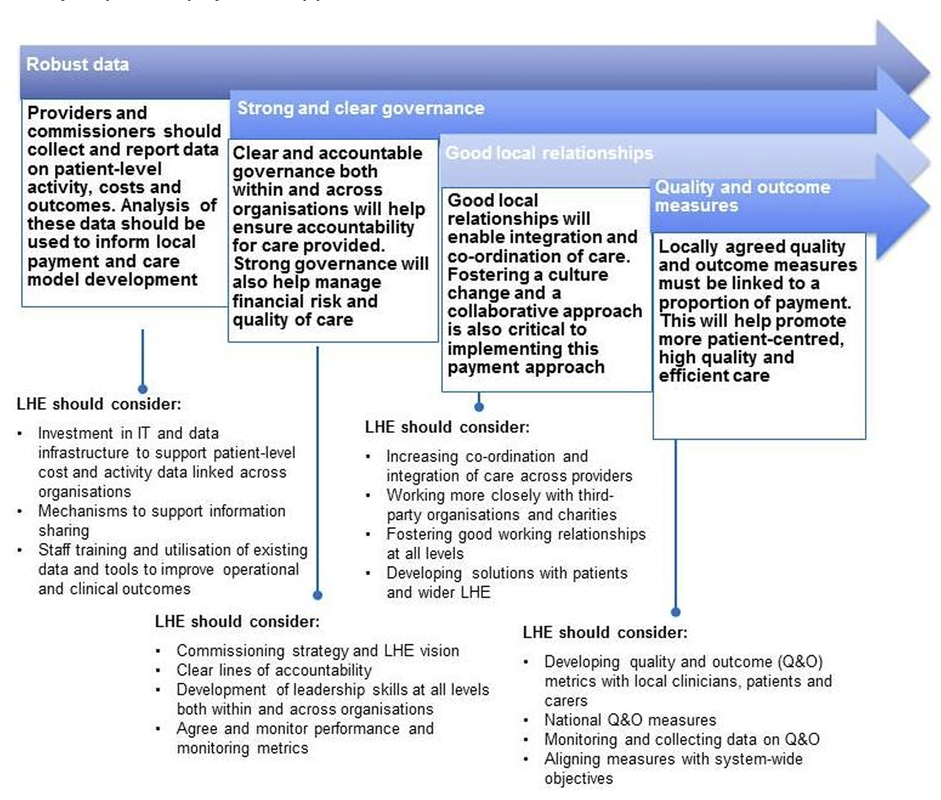
What are the components needed to develop a capitated payment approach for mental health?
The scope of care covered by capitated payment, and contractual arrangements underpinning capitated payment, may vary depending on local factors. Factors to take into account may include the degree of co-ordination between mental healthcare and other services, and/or on the robustness of data. When developing local capitated payment arrangements, the seven steps described below need to be followed. Where more than one mental health organisation is responsible for delivering a capitated contract, a lead provider who holds the capitated budget must be agreed. This lead provider then works with each of the other (delivery) partners to deliver care.
Commissioners will need to use an appropriate process to decide which provider is best placed to be the lead provider. Commissioners can contact Monitor for support in ensuring this process delivers good outcomes for patients and is consistent with the Procurement, Patient Choice and Competition Regulations.
The scope of care covered by capitated payment, and contractual arrangements underpinning capitated payment, may vary depending on local factors. Factors to take into account may include the degree of co-ordination between mental healthcare and other services, and/or on the robustness of data. When developing local capitated payment arrangements, the seven steps described below need to be followed. Where more than one mental health organisation is responsible for delivering a capitated contract, a lead provider who holds the capitated budget must be agreed. This lead provider then works with each of the other (delivery) partners to deliver care.
Commissioners will need to use an appropriate process to decide which provider is best placed to be the lead provider. Commissioners can contact Monitor for support in ensuring this process delivers good outcomes for patients and is consistent with the Procurement, Patient Choice and Competition Regulations.
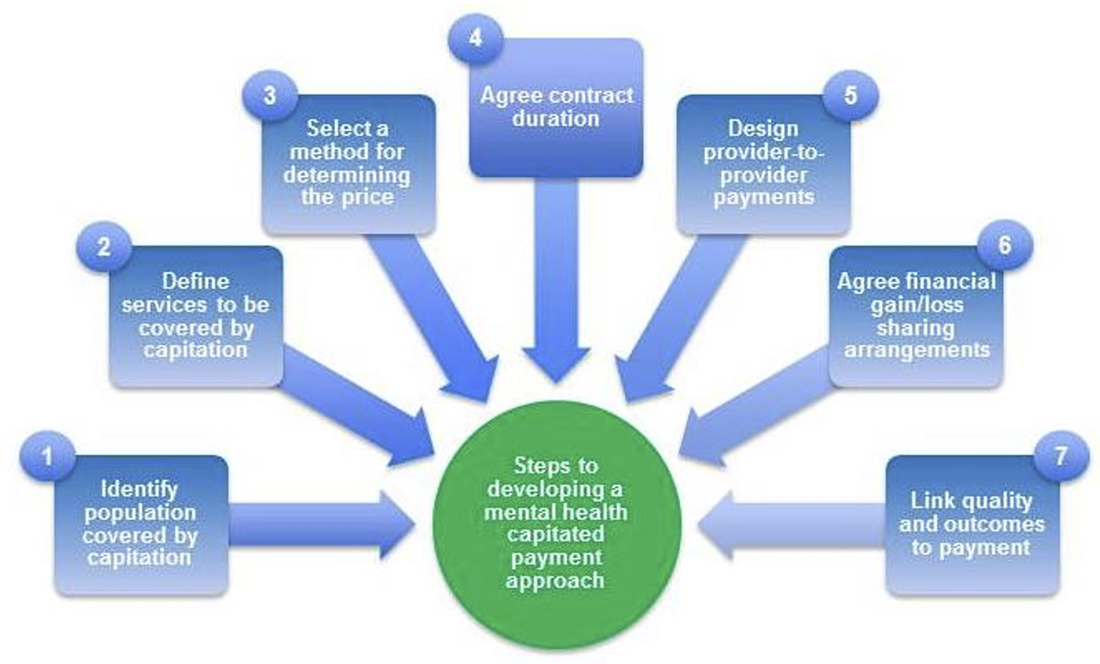
Step 1: Identify the population to be covered by capitation
Providers and commissioners must identify the adult and older people’s cohort to be included in the capitated payment for mental healthcare. They may consider including other population cohorts (eg children) as well as provision of other health and social care under a capitated payment. GP registration lists should be used to identify the population for capitation. However, not everyone is registered with a GP and other data are needed to identify the population to be covered by the capitated payment. and to understand unmet need and the potential demand for mental health services. The points to consider listed in the table below illustrate why a combination of GP registration lists and referral lists is best for the identification of the population to be covered by capitation.
GP registration lists
Strongly incentivise the capitated budget holder to undertake early intervention and prevention (ie to avoid referrals to more expensive secondary mental health services)
This better captures unmet patient demand than looking only at secondary mental health provider activity
Lists are relatively large, and therefore capture a large proportion of the LHE
Providers need to ensure that they can manage the demand for services covered by capitation from those whose needs may not have been previously met
People referred to secondary mental health services
Provides a more focused identification of the local population that may need mental healthcare
Reduces risk of transferring insurance risk to provider
Need to consider how service users access services, as some self-refer without a GP referral. Service entry points need to be clearly defined so that there is no restriction of access to care
Does not strongly incentivise early intervention and prevention
Likely to cover a smaller population and less likely to capture wider MH care needs in the LHE
To determine the potential demand for mental health services in the target population, it is also important to understand the levels of unmet need in this population. This should include assessment of other data may include Office for National Statistics data, emergency services data and referrals to secondary mental health services.
Step 2: Define services to be covered by capitation
Providers and commissioners must work together to specify the scope of services, in collaboration with people with mental ill health, carers, clinicians and also other interested organisations (eg local authorities). The scope of services should be based on clinical guidance and evidenced-based care, and support agreed quality and outcome measures. The scope of services included in a capitated payment will depend on the LHE characteristics and needs of the population to be covered. LHEs should include mental healthcare for adult and older people in the capitated payment, but also some aspects of physical, social and community care. This widening of the scope of services is particularly important given the strong clinical interrelationship between mental and physical ill health for recovery and wellness. Therefore, co-ordinated care benefits both people with mental ill health, and system efficiency by ensuring care is co-ordinated effectively. Similarly, it may be appropriate for the capitated payment to cover other mental healthcare (eg children’s mental healthcare and/or specialised mental healthcare for adults). The scope of services should apply to the whole population covered by capitation, but additional care/interventions can be specified for a subset of the population; for example, people with dementia or serious mental illness.
Providers and commissioners must identify the adult and older people’s cohort to be included in the capitated payment for mental healthcare. They may consider including other population cohorts (eg children) as well as provision of other health and social care under a capitated payment. GP registration lists should be used to identify the population for capitation. However, not everyone is registered with a GP and other data are needed to identify the population to be covered by the capitated payment. and to understand unmet need and the potential demand for mental health services. The points to consider listed in the table below illustrate why a combination of GP registration lists and referral lists is best for the identification of the population to be covered by capitation.
GP registration lists
Strongly incentivise the capitated budget holder to undertake early intervention and prevention (ie to avoid referrals to more expensive secondary mental health services)
This better captures unmet patient demand than looking only at secondary mental health provider activity
Lists are relatively large, and therefore capture a large proportion of the LHE
Providers need to ensure that they can manage the demand for services covered by capitation from those whose needs may not have been previously met
People referred to secondary mental health services
Provides a more focused identification of the local population that may need mental healthcare
Reduces risk of transferring insurance risk to provider
Need to consider how service users access services, as some self-refer without a GP referral. Service entry points need to be clearly defined so that there is no restriction of access to care
Does not strongly incentivise early intervention and prevention
Likely to cover a smaller population and less likely to capture wider MH care needs in the LHE
To determine the potential demand for mental health services in the target population, it is also important to understand the levels of unmet need in this population. This should include assessment of other data may include Office for National Statistics data, emergency services data and referrals to secondary mental health services.
Step 2: Define services to be covered by capitation
Providers and commissioners must work together to specify the scope of services, in collaboration with people with mental ill health, carers, clinicians and also other interested organisations (eg local authorities). The scope of services should be based on clinical guidance and evidenced-based care, and support agreed quality and outcome measures. The scope of services included in a capitated payment will depend on the LHE characteristics and needs of the population to be covered. LHEs should include mental healthcare for adult and older people in the capitated payment, but also some aspects of physical, social and community care. This widening of the scope of services is particularly important given the strong clinical interrelationship between mental and physical ill health for recovery and wellness. Therefore, co-ordinated care benefits both people with mental ill health, and system efficiency by ensuring care is co-ordinated effectively. Similarly, it may be appropriate for the capitated payment to cover other mental healthcare (eg children’s mental healthcare and/or specialised mental healthcare for adults). The scope of services should apply to the whole population covered by capitation, but additional care/interventions can be specified for a subset of the population; for example, people with dementia or serious mental illness.
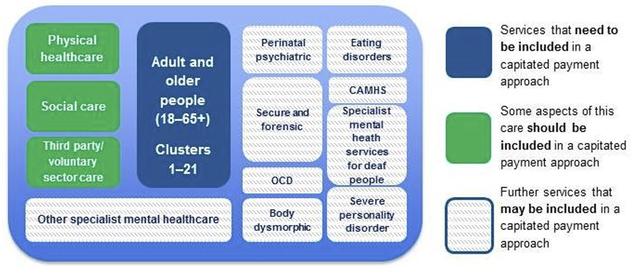
Possible in-scope services are outlined below.
Providers and commissioners may include mechanisms that help the capitated budget holder to better manage financial risk. For example, specific (expensive but infrequent) care for people with mental ill health can be excluded from the payment arrangement (eg care for those in high secure units).
Step 3: Select a method for determining the price per person per year Current commissioner spend is used as the starting point for the calculation, but the following three factors all need to be taken into account when determining the capitated payment:
1. Existing baseline spend on mental healthcare and adjustments for the (actual) baseline cost of provision incurred by providers.
2. Adjustments to the overall payment based on forecast need and associated costs:
financial impact of putting in place, potentially new, effective and efficient clinical models that meet the needs of the population, including the delivery of NICE-concordant care
year-on-year adjustments to reflect expected changes, eg population/casemix changes, cost inflation, efficiency savings
possible adjustment to reflect the cost of providing care to those who have been assessed and are on a waiting list, as well as those whose need is as yet unidentified. This requires analysis of a number of information sources, such as mental health risk stratification tools (eg from Public Health England), and engagement with other local services (eg emergency services, education and local government).
3. Where a multi-year arrangement is agreed, in future years, adjustments can be based on actual outturn given that the forecasts are unlikely to be accurate over the entire period.
Step 4: Agree contract duration Providers and commissioners must agree upfront the duration of the capitated contract. This should be long enough to realise the potential benefits to people with mental ill health and the wider LHE. Providers and commissioners should ensure that any agreed contract is consistent with the local payment rules.
Step 5: Design provider-to-provider payment mechanisms Where a provider subcontracts the delivery of care to other providers, it is important to agree a clear and robust provider-to-provider payment mechanism. In the case of a capitated payment focused on mental healthcare provision, payment would be made to a lead/accountable provider, which may then make subcontract arrangements with other providers of mental healthcare and related services. The subcontracted payment arrangements would vary depending on the incentives that need to be created by the lead provider, as well as the nature and duration of the contract. An example of how a lead provider could work with other subcontracted providers is given below.
Step 3: Select a method for determining the price per person per year Current commissioner spend is used as the starting point for the calculation, but the following three factors all need to be taken into account when determining the capitated payment:
1. Existing baseline spend on mental healthcare and adjustments for the (actual) baseline cost of provision incurred by providers.
2. Adjustments to the overall payment based on forecast need and associated costs:
financial impact of putting in place, potentially new, effective and efficient clinical models that meet the needs of the population, including the delivery of NICE-concordant care
year-on-year adjustments to reflect expected changes, eg population/casemix changes, cost inflation, efficiency savings
possible adjustment to reflect the cost of providing care to those who have been assessed and are on a waiting list, as well as those whose need is as yet unidentified. This requires analysis of a number of information sources, such as mental health risk stratification tools (eg from Public Health England), and engagement with other local services (eg emergency services, education and local government).
3. Where a multi-year arrangement is agreed, in future years, adjustments can be based on actual outturn given that the forecasts are unlikely to be accurate over the entire period.
Step 4: Agree contract duration Providers and commissioners must agree upfront the duration of the capitated contract. This should be long enough to realise the potential benefits to people with mental ill health and the wider LHE. Providers and commissioners should ensure that any agreed contract is consistent with the local payment rules.
Step 5: Design provider-to-provider payment mechanisms Where a provider subcontracts the delivery of care to other providers, it is important to agree a clear and robust provider-to-provider payment mechanism. In the case of a capitated payment focused on mental healthcare provision, payment would be made to a lead/accountable provider, which may then make subcontract arrangements with other providers of mental healthcare and related services. The subcontracted payment arrangements would vary depending on the incentives that need to be created by the lead provider, as well as the nature and duration of the contract. An example of how a lead provider could work with other subcontracted providers is given below.

Step 6: Agree financial gain/loss sharing arrangements
Any gain/loss sharing mechanism6 must align with the system-wide objectives and allocate financial risk appropriately. Providers and commissioners should agree in advance how, and to what extent, any financial gain or loss is shared between them. It may also be desirable to link all providers under one gain/loss sharing arrangement with a commissioner(s), particularly where co-ordinated care is being delivered. The proportion of financial gain that is shared with any provider(s) should be sufficient to incentivise their delivery of high quality care and innovation. The proportion of financial loss that is shared should be agreed in advance, and must not negatively impact the quality of care. It may also be possible to phase in gain/loss sharing arrangements to allow providers to transition to the new payment approach. For example, in the first phase financial gains only could be shared and these used to invest in infrastructure and training. The second phase could entail providers sharing both financial gains and losses.
Step 7: Link quality and outcomes to payment
In any capitated payment approach providers and commissioners must identify and link payment to quality and outcomes metrics, which will influence the final payment made to the provider(s). This can ensure providers do not sacrifice quality and patient outcomes to generate financial savings. Providers and commissioners must identify the quality and outcomes measures to link to payment. These should include the national measures for mental healthcare that are being developed, but locally determined measures will also be needed. Local measures should be co-developed with all important local stakeholders, ie service users, clinicians, providers and commissioners, and reflect evidence-based approaches to care and National Institute for Health and Care Excellence (NICE) guidance. Monitor and NHS England will provide further guidance on using and developing quality and outcomes measures, and how these can be linked to payment.
Further resources This short guide is one in a series of publications to help support the sector develop payment approaches for mental health.7
© Monitor (December 2015) Publication code: IRG 42/15
NHS England Publications Gateway Reference 04463
NHS England Document Classification: Official
Any gain/loss sharing mechanism6 must align with the system-wide objectives and allocate financial risk appropriately. Providers and commissioners should agree in advance how, and to what extent, any financial gain or loss is shared between them. It may also be desirable to link all providers under one gain/loss sharing arrangement with a commissioner(s), particularly where co-ordinated care is being delivered. The proportion of financial gain that is shared with any provider(s) should be sufficient to incentivise their delivery of high quality care and innovation. The proportion of financial loss that is shared should be agreed in advance, and must not negatively impact the quality of care. It may also be possible to phase in gain/loss sharing arrangements to allow providers to transition to the new payment approach. For example, in the first phase financial gains only could be shared and these used to invest in infrastructure and training. The second phase could entail providers sharing both financial gains and losses.
Step 7: Link quality and outcomes to payment
In any capitated payment approach providers and commissioners must identify and link payment to quality and outcomes metrics, which will influence the final payment made to the provider(s). This can ensure providers do not sacrifice quality and patient outcomes to generate financial savings. Providers and commissioners must identify the quality and outcomes measures to link to payment. These should include the national measures for mental healthcare that are being developed, but locally determined measures will also be needed. Local measures should be co-developed with all important local stakeholders, ie service users, clinicians, providers and commissioners, and reflect evidence-based approaches to care and National Institute for Health and Care Excellence (NICE) guidance. Monitor and NHS England will provide further guidance on using and developing quality and outcomes measures, and how these can be linked to payment.
Further resources This short guide is one in a series of publications to help support the sector develop payment approaches for mental health.7
© Monitor (December 2015) Publication code: IRG 42/15
NHS England Publications Gateway Reference 04463
NHS England Document Classification: Official
Payment by results: validating care cluster allocation in the real world
Stavros Bekas, Orlin Michev
The Psychiatrist (2013), 37, 349-355
Introduction
The financial year 2012–13 witnessed a major change in the way that mental healthcare is funded, a shift from block contracts to payment by results (PbR) ‘currencies’. These have been in use in acute care for years and are linked to ICD-10 codes and unit costs for procedures and treatments. Acute PbR was founded on the strategic priorities set by the
National Service Framework policy launched in 2000 which included structural transformations in combination with financial ‘levers for change’. Introducing PbR currencies was the Department of Health’s chosen approach for the interface between commissioners and providers.
Payment by results in mental health will be significantly different in that it will not use fixed tariffs for each condition; rather, payment will be linked with individual patient needs and care plans produced during their contact with mental health services. It was decided to produce currencies through the allocation of patients to 21 ‘clusters’ of care using the Mental Health Clustering Tool (MHCT). A cluster corresponds to a group of patients with similar clinical symptoms, needs and disabilities, with the idea that a single tariff on average will be sufficient to cover the cost of care for each patient allocated to the cluster. Mental health PbR has been enshrined as a commitment for the Department of Health and National Health Service (NHS) providers in the government’s White Paper Liberating the NHS.4 Current policy envisages the introduction of local prices which will form the basis of commissioning contracts in 2013-14, and the earliest date for introduction of national prices is set to be in 2015. Guidance for mental health PbR recognises that local cluster allocation quality and quantity information for 2013-14 will continue to be variable and suggests that providers and commissioners should ‘work together to
mitigate the risks of financial instability’.
Discussion
A report by the Sainsbury Centre for Mental Health raised concerns about the challenges that PbR presented in mental health, as this approach is characterised by long-term and episodic conditions, variability of services and the cost of care is influenced by a multitude of factors beyond diagnosis (i.e. multi-agency pathways and informal care). Dangers of
acute PbR have been established through many years of international experience – that providers may ‘cherry pick’ easier and cheaper cases, reduce quality of care by hastening turnover, manipulate patient coding into higher tariffs or increase activity to such an extent that commissioners cannot afford the cost. As a result, it was suggested not to abandon PbR altogether, but to include safeguards that improve coding, prevent excessive hospital utilisation and promote quality of care.
Similarly, problems identified by the developers of mental health PbR currencies included lack of a satisfactory classification system, large provider variations, case-mix of acute and chronic cases and variable care needs, in addition to major technical challenges in auditing and data collection. The same developers later acknowledged the lack of robust evidence to further support the ‘high face validity’ of clusters and failed to demonstrate beyond doubt that they constitute a ‘fit for purpose classification system’, attributing the difficulty to data quality and methodological difficulties.
Achieving homogeneity within clusters is considered essential to ensure that PbR will not introduce financial risk for providers. This was the primary reason why similar approaches to payment were not implemented for mental health services in the USA, Australia or New Zealand. Similarly, initial cost analyses in the UK demonstrated that
homogeneity within clusters was ‘unacceptably low’ and that providers vary in their resource utilisation much more than
what could be explained by differences in their case-load.
Arguably, PbR challenges are multiplied by the fact that we are currently facing the most extensive financial retrenching since the introduction of the internal market in the NHS, in combination with a drive for quality improvement and patient choice. Payment by results was heralded as the mechanism by which payment is attached to patient choices, but the Department of Health also aimed to provide incentives to providers to achieve the lowest cost consistent with quality outcomes, while the tools from which the MHCT is derived and the process of defining clusters did not take into account costs at all. Later work replicated the significant problems in having quality data and in including outcomes as a means of incentivising quality improvement. Nevertheless, PbR remains an opportunity to have more transparent commissioning and potentially can act as a strong incentive for the routine recording of clinical outcomes, and may encourage clinical involvement in financial management.
Main findings
The study provided evidence of potentially unacceptable levels of inappropriate allocation to care clusters, raising concerns about the readiness to fully implement the next stages of mental health PbR.
This study provides evidence of how imprecise the allocation of patients with personality disorder is... It is possible that common practice is to reserve a diagnosis of personality disorder for the most extreme cases and instead give a diagnosis of affective disorder. Similar issues with failure to record all the applicable diagnoses explain most of the mismatch for the
comorbid conditions.
The study also provides evidence that the results of the validation varied greatly depending on the methodology used. The vast majority of errors picked by the automated cross-check with ICD-10 codes proved to be genuine misallocations and were not justified on clinical grounds.
These results provide evidence that as a result of the inherent design of the MHCT, scores alone cannot be used for error-free, reliable allocation to clusters and corresponding care packages. Conversely, a more holistic and iterative, rather than a linear and algorithmic, approach would be more reliable. Lately, an increasing number of voices have called for the inclusion of diagnosis and care package descriptions as a more accurate approach to costing. Diagnostic systems such as the ICD-10 have been developed after many years of rigorous research and international consensus, and have proven classification properties. Diagnostic labels tend to remain the same over time. They convey a great deal of clinically
useful information and are already widely recorded in data-sets in trusts and provided to commissioners and the Department
of Health. An additional argument for the inclusion of diagnosis in PbR is that current training, research, evidence based
guidelines, such as those by the National Institute for Health and Care Excellence, and service configurations so far have been primarily based on diagnoses. It is stressed within the principles of the clustering guidance that the final arbiter in allocating a PbR cluster should always be clinical judgement, which can be better informed by a combination of diagnosis, MHCT and other rating tool scores, and the best match from an array of available packages of care.
The use of ICD-10 diagnosis appears more reliable than using the HoNOS/MHCT scores to audit practice. On the other hand, comparing against diagnostic codes is not validation in the classic sense, as there is no evidence that recorded ICD-10 codes are fully reliable. The absence of a true ‘gold standard’ in this case makes necessary the use of comparison and triangulation methods as those described here, preferably using the combination of both ICD-10 codes and HoNOS/MHCT scores as the most rigorous approach in auditing cluster allocation by clinical staff.
Stavros Bekas, Orlin Michev
The Psychiatrist (2013), 37, 349-355
Introduction
The financial year 2012–13 witnessed a major change in the way that mental healthcare is funded, a shift from block contracts to payment by results (PbR) ‘currencies’. These have been in use in acute care for years and are linked to ICD-10 codes and unit costs for procedures and treatments. Acute PbR was founded on the strategic priorities set by the
National Service Framework policy launched in 2000 which included structural transformations in combination with financial ‘levers for change’. Introducing PbR currencies was the Department of Health’s chosen approach for the interface between commissioners and providers.
Payment by results in mental health will be significantly different in that it will not use fixed tariffs for each condition; rather, payment will be linked with individual patient needs and care plans produced during their contact with mental health services. It was decided to produce currencies through the allocation of patients to 21 ‘clusters’ of care using the Mental Health Clustering Tool (MHCT). A cluster corresponds to a group of patients with similar clinical symptoms, needs and disabilities, with the idea that a single tariff on average will be sufficient to cover the cost of care for each patient allocated to the cluster. Mental health PbR has been enshrined as a commitment for the Department of Health and National Health Service (NHS) providers in the government’s White Paper Liberating the NHS.4 Current policy envisages the introduction of local prices which will form the basis of commissioning contracts in 2013-14, and the earliest date for introduction of national prices is set to be in 2015. Guidance for mental health PbR recognises that local cluster allocation quality and quantity information for 2013-14 will continue to be variable and suggests that providers and commissioners should ‘work together to
mitigate the risks of financial instability’.
Discussion
A report by the Sainsbury Centre for Mental Health raised concerns about the challenges that PbR presented in mental health, as this approach is characterised by long-term and episodic conditions, variability of services and the cost of care is influenced by a multitude of factors beyond diagnosis (i.e. multi-agency pathways and informal care). Dangers of
acute PbR have been established through many years of international experience – that providers may ‘cherry pick’ easier and cheaper cases, reduce quality of care by hastening turnover, manipulate patient coding into higher tariffs or increase activity to such an extent that commissioners cannot afford the cost. As a result, it was suggested not to abandon PbR altogether, but to include safeguards that improve coding, prevent excessive hospital utilisation and promote quality of care.
Similarly, problems identified by the developers of mental health PbR currencies included lack of a satisfactory classification system, large provider variations, case-mix of acute and chronic cases and variable care needs, in addition to major technical challenges in auditing and data collection. The same developers later acknowledged the lack of robust evidence to further support the ‘high face validity’ of clusters and failed to demonstrate beyond doubt that they constitute a ‘fit for purpose classification system’, attributing the difficulty to data quality and methodological difficulties.
Achieving homogeneity within clusters is considered essential to ensure that PbR will not introduce financial risk for providers. This was the primary reason why similar approaches to payment were not implemented for mental health services in the USA, Australia or New Zealand. Similarly, initial cost analyses in the UK demonstrated that
homogeneity within clusters was ‘unacceptably low’ and that providers vary in their resource utilisation much more than
what could be explained by differences in their case-load.
Arguably, PbR challenges are multiplied by the fact that we are currently facing the most extensive financial retrenching since the introduction of the internal market in the NHS, in combination with a drive for quality improvement and patient choice. Payment by results was heralded as the mechanism by which payment is attached to patient choices, but the Department of Health also aimed to provide incentives to providers to achieve the lowest cost consistent with quality outcomes, while the tools from which the MHCT is derived and the process of defining clusters did not take into account costs at all. Later work replicated the significant problems in having quality data and in including outcomes as a means of incentivising quality improvement. Nevertheless, PbR remains an opportunity to have more transparent commissioning and potentially can act as a strong incentive for the routine recording of clinical outcomes, and may encourage clinical involvement in financial management.
Main findings
The study provided evidence of potentially unacceptable levels of inappropriate allocation to care clusters, raising concerns about the readiness to fully implement the next stages of mental health PbR.
This study provides evidence of how imprecise the allocation of patients with personality disorder is... It is possible that common practice is to reserve a diagnosis of personality disorder for the most extreme cases and instead give a diagnosis of affective disorder. Similar issues with failure to record all the applicable diagnoses explain most of the mismatch for the
comorbid conditions.
The study also provides evidence that the results of the validation varied greatly depending on the methodology used. The vast majority of errors picked by the automated cross-check with ICD-10 codes proved to be genuine misallocations and were not justified on clinical grounds.
These results provide evidence that as a result of the inherent design of the MHCT, scores alone cannot be used for error-free, reliable allocation to clusters and corresponding care packages. Conversely, a more holistic and iterative, rather than a linear and algorithmic, approach would be more reliable. Lately, an increasing number of voices have called for the inclusion of diagnosis and care package descriptions as a more accurate approach to costing. Diagnostic systems such as the ICD-10 have been developed after many years of rigorous research and international consensus, and have proven classification properties. Diagnostic labels tend to remain the same over time. They convey a great deal of clinically
useful information and are already widely recorded in data-sets in trusts and provided to commissioners and the Department
of Health. An additional argument for the inclusion of diagnosis in PbR is that current training, research, evidence based
guidelines, such as those by the National Institute for Health and Care Excellence, and service configurations so far have been primarily based on diagnoses. It is stressed within the principles of the clustering guidance that the final arbiter in allocating a PbR cluster should always be clinical judgement, which can be better informed by a combination of diagnosis, MHCT and other rating tool scores, and the best match from an array of available packages of care.
The use of ICD-10 diagnosis appears more reliable than using the HoNOS/MHCT scores to audit practice. On the other hand, comparing against diagnostic codes is not validation in the classic sense, as there is no evidence that recorded ICD-10 codes are fully reliable. The absence of a true ‘gold standard’ in this case makes necessary the use of comparison and triangulation methods as those described here, preferably using the combination of both ICD-10 codes and HoNOS/MHCT scores as the most rigorous approach in auditing cluster allocation by clinical staff.
Clustering in mental health payment by results: a critical summary for the clinician
David Yeomans
Advances in psychiatric treatment (2014), vol. 20, 227–234
Summary
Mental health payment by results (PbR) is a disruptive new prospective payment system intended to replace National Health Service block contracts in England and provide a mechanism for opening up the mental health economy. Patients are allocated to one of 21 treatment clusters, each with a different price or tariff. Clinicians perform cluster allocation using the Mental Health Clustering Tool. The clustering process makes demands on clinicians’ time even with support from information systems. Clustering is novel and it is unclear how it will work in practice. The process is likely to be susceptible to gaming.
Learning objectives
• Understand that the clinical process of diagnostic classification is different from the financial process of clustering categorisation.
• Understand the importance of learning the clustering tool ratings definitions in order to make accurate cluster allocations.
• Recognise that mental health payment by results is driving the widespread adoption of outcomes measurement.
Mental health payment by results (PbR) is precisely the sort of mechanism that Adam Smith recommended almost 340 years ago to fund public services. It is a financial device that can be used or misused, depending on your orientation, in a
variety of ways that this article will explore. A companion article in Advances by Rowena Jacobs describes PbR systems in detail (Jacobs 2014). The purpose of mental health PbR is to effect change. Currently, psychiatric services in England
are paid for with block contracts that do not vary according to activity. Adam Smith recommended that public services are reimbursed in proportion to the volume of activity performed and this is what mental health PbR aims to do.
Clustering and outcome measures
Despite the name, mental health PbR does not yet pay on the basis of results or outcomes, but by activity. Not all activity is of the same nature or degree, so the authors of mental health PbR have developed a currency to address case mix.
Thus, more demanding provision is funded at a higher level than less complex or intense work. This case-mix approach is called clustering. It is the equivalent of healthcare resource groups in other systems.
Mental health clusters are assigned using the Mental Health Clustering Tool (MHCT), a structured rating of behaviour, symptoms, risk, functional status and history. When clinicians assign a cluster to a patient they are allocating a fixed price for that patient’s care for a set period of time called a cluster review period. Any qualified provider of mental health services can bid to offer a service to a patient at that fixed price. Providers that spend less on service provision than the cluster tariff will make a profit, and those spending more will lose money. The system therefore encourages providers to work within the
price limit of each cluster, and it is hoped that this will drive down the costs of service provision. Of course, there have to be checks and balances to encourage quality as well as efficiency. In future, various forms of outcome measure will be used to
help determine quality.
The administrative burden of clustering Clinicians may be diverted somewhat from direct patient care by clustering, which is a process equivalent to raising invoices in a retrospective payment system. This diversion may increase as demands for quality measures and outcomes are included. Computerised administrative systems could offer support to minimise loss of productivity, and staff will need to adapt to the new environment. In acute services, PbR is supported by administrative staff called clinical coders. Clinicians record diagnoses and procedures and then the coders transform these into tariff codes.
This separation of clinicians from accounting means that they are unlikely to be drawn into gaming the system, a protection that mental health PbR does not afford. In mental health PbR, the clinicians are also the coders.
Diagnosis and clustering processes are not the same
Clustering will make all professional groups in mental healthcare adopt a new classification system to support the flow of money around the National Health Service (NHS). Doctors in particular need to understand that this new financial classification system differs from diagnostic systems. Clusters borrow heavily from the clinical language of medical diagnosis, but they have very different meanings. When a practitioner makes a clinical judgement that someone has a
first-episode psychosis this is because the person reports a syndrome of psychotic symptoms such as hallucinations and delusions, and is experiencing distress and disability. When the same practitioner allocates the same person to a mental health cluster called first-episode psychosis they do so in order to receive payment of £10 606 during that cluster’s review period of 12 months. Clustering is a financial process wrapped up in clinical terms.
The Royal College of Psychiatrists (2014) does not support the current clustering model. The College position statement on mental health payment systems expresses dissatisfaction that diagnosis is a secondary consideration to the clustering system. College members are concerned that ‘the implementation of the current system would risk severe destabilisation, both financially and organisationally’. Perhaps the absence of diagnosis challenges the position of psychiatrists in the system.
Making a diagnosis is a process of using information gained from conversations and examinations to categorise people into groups. It is a fundamental part of the medical model. In psychiatry there is little pathological evidence to inform diagnoses, so the profession has developed diagnostic standards, based on clinical assessments, published as international diagnostic
manuals. The system of allocating clusters is a different categorisation process, with 21 clusters instead of several hundred diagnoses. Clustering does not use diagnosis because diagnosis is not well correlated with mental healthcare expenditure – other factors, such as marital status and electoral ward of residence, are better predictors of cost (Oyebode 2007).
The MHCT relies in large part on a set of scales developed by the Royal College of Psychiatrists’ Research Unit in the 1990s called the Health of the Nation Outcome Scales (HoNOS) (Wing 1996), so it does have clinical credentials, but
there is no scheme to translate backwards and forwards between diagnosis and clustering. A person with a diagnosis of first-episode psychosis could be allocated to one of several clusters, such as ‘psychotic crisis’, ‘first-episode psychosis’ or
‘ongoing or recurrent psychosis (high symptom and disability)’. A person with a cluster allocation of ‘psychotic crisis’ may have a clinical diagnosis of schizophrenia, mania, depression or personality disorder. The cluster is a single price that
covers all psychiatric comorbidities in a single category. A person with multiple psychiatric diagnoses (e.g. depression, substance misuse and personality disorder) will only receive one mental health cluster.
Gaming
Financial incentives change behaviour. The behaviour that organisations and individuals engage in to maximise income is sometimes called gaming. General practitioner commissioners have complained that trusts in acute physical care game their PbR systems. Gaming can create perverse activity. For example, some trusts facing financial penalties for failing to meet 4-hour waiting time targets in accident and emergency (A & E) departments apparently made patients wait outside in ambulances so as to delay the actual entry to A & E, when the clock starts ticking.
Up-coding
Financial gaming is limited with block budgets that are remote from clinicians, but mental healthcare practitioners using PbR will be immersed in the financial process. With PbR, each patient has a regular financial assessment by a clinician, who assigns a price to the patient. Practitioners usually want to get the best service for their patients and may tweak their clustering tool ratings up a bit to achieve a higher-paying cluster. This will be easy to do as they become familiar with the idiosyncrasies of the clustering algorithm. As a result, clinicians might assign more patients to high-value clusters (this is called up-coding and increases income without increasing quality). It is likely that internal and external audit processes (another cost) will be needed to monitor systematic up- or down-coding.
Cream-skimming and dumping
Service providers may decide to reorganise their services to include only simple, predictable cases that bring in a steady income (sometimes called cream-skimming), leaving patients with more complex needs (and higher financial risks) with
less input (dumping).
Combatting gaming
Organisational and clinical entrepreneurs will use the PbR system to their advantage, so it is very important that there are clear measures of patient benefit and harm to make sure that patients do not lose out. Some of these measures need to be independent of the MHCT, since gaming of the tool for income necessarily would game the outcome derived from HoNOS. Up-coding on initial assessment both increases income and inflates future positive outcomes, so there is a double incentive to exaggerate cluster assignments. Although CROMs have value, it may be the PROMs and PREMs that are the most independent and transparent.
Summary
Mental health PbR and clustering constitute a highly disruptive financial mechanism for funding mental healthcare that brings the NHS closer to a market approach. There are still many challenges ahead and it is quite possible that mental health PbR may not work out. The purchaser/provider split is not a panacea for service improvement, and
state-funded services can increase efficiency and quality without it (Timmins 2013).
Implementation has been put back more than once, but mental health PbR still appears to be on the way and services need to be prepared. Clustering will reduce clinical time for patients, but the impact can be lessened with good IT support and good training. Gaming will be easy and should be discouraged from the outset by emphasising probity and professionalism. Outcome measures will be introduced and these could help patients and practitioners understand what kind of care really works.
New providers, including big business and the voluntary sector, can enter the market. Small independent providers and individuals could benefit because they may be able to access money currently bound up in block contracts. There
will also be losers in a market approach. Among service providers, the losers could be those that do not upgrade their IT systems and those that fail to engage and train their staff. Many clinicians just want to get on with their primary jobs. For
them, the best approach to clustering is to try to do it accurately and quickly. The Care Pathways & Packages Project (CPPP) is developing the clustering currency.
David Yeomans
Advances in psychiatric treatment (2014), vol. 20, 227–234
Summary
Mental health payment by results (PbR) is a disruptive new prospective payment system intended to replace National Health Service block contracts in England and provide a mechanism for opening up the mental health economy. Patients are allocated to one of 21 treatment clusters, each with a different price or tariff. Clinicians perform cluster allocation using the Mental Health Clustering Tool. The clustering process makes demands on clinicians’ time even with support from information systems. Clustering is novel and it is unclear how it will work in practice. The process is likely to be susceptible to gaming.
Learning objectives
• Understand that the clinical process of diagnostic classification is different from the financial process of clustering categorisation.
• Understand the importance of learning the clustering tool ratings definitions in order to make accurate cluster allocations.
• Recognise that mental health payment by results is driving the widespread adoption of outcomes measurement.
Mental health payment by results (PbR) is precisely the sort of mechanism that Adam Smith recommended almost 340 years ago to fund public services. It is a financial device that can be used or misused, depending on your orientation, in a
variety of ways that this article will explore. A companion article in Advances by Rowena Jacobs describes PbR systems in detail (Jacobs 2014). The purpose of mental health PbR is to effect change. Currently, psychiatric services in England
are paid for with block contracts that do not vary according to activity. Adam Smith recommended that public services are reimbursed in proportion to the volume of activity performed and this is what mental health PbR aims to do.
Clustering and outcome measures
Despite the name, mental health PbR does not yet pay on the basis of results or outcomes, but by activity. Not all activity is of the same nature or degree, so the authors of mental health PbR have developed a currency to address case mix.
Thus, more demanding provision is funded at a higher level than less complex or intense work. This case-mix approach is called clustering. It is the equivalent of healthcare resource groups in other systems.
Mental health clusters are assigned using the Mental Health Clustering Tool (MHCT), a structured rating of behaviour, symptoms, risk, functional status and history. When clinicians assign a cluster to a patient they are allocating a fixed price for that patient’s care for a set period of time called a cluster review period. Any qualified provider of mental health services can bid to offer a service to a patient at that fixed price. Providers that spend less on service provision than the cluster tariff will make a profit, and those spending more will lose money. The system therefore encourages providers to work within the
price limit of each cluster, and it is hoped that this will drive down the costs of service provision. Of course, there have to be checks and balances to encourage quality as well as efficiency. In future, various forms of outcome measure will be used to
help determine quality.
The administrative burden of clustering Clinicians may be diverted somewhat from direct patient care by clustering, which is a process equivalent to raising invoices in a retrospective payment system. This diversion may increase as demands for quality measures and outcomes are included. Computerised administrative systems could offer support to minimise loss of productivity, and staff will need to adapt to the new environment. In acute services, PbR is supported by administrative staff called clinical coders. Clinicians record diagnoses and procedures and then the coders transform these into tariff codes.
This separation of clinicians from accounting means that they are unlikely to be drawn into gaming the system, a protection that mental health PbR does not afford. In mental health PbR, the clinicians are also the coders.
Diagnosis and clustering processes are not the same
Clustering will make all professional groups in mental healthcare adopt a new classification system to support the flow of money around the National Health Service (NHS). Doctors in particular need to understand that this new financial classification system differs from diagnostic systems. Clusters borrow heavily from the clinical language of medical diagnosis, but they have very different meanings. When a practitioner makes a clinical judgement that someone has a
first-episode psychosis this is because the person reports a syndrome of psychotic symptoms such as hallucinations and delusions, and is experiencing distress and disability. When the same practitioner allocates the same person to a mental health cluster called first-episode psychosis they do so in order to receive payment of £10 606 during that cluster’s review period of 12 months. Clustering is a financial process wrapped up in clinical terms.
The Royal College of Psychiatrists (2014) does not support the current clustering model. The College position statement on mental health payment systems expresses dissatisfaction that diagnosis is a secondary consideration to the clustering system. College members are concerned that ‘the implementation of the current system would risk severe destabilisation, both financially and organisationally’. Perhaps the absence of diagnosis challenges the position of psychiatrists in the system.
Making a diagnosis is a process of using information gained from conversations and examinations to categorise people into groups. It is a fundamental part of the medical model. In psychiatry there is little pathological evidence to inform diagnoses, so the profession has developed diagnostic standards, based on clinical assessments, published as international diagnostic
manuals. The system of allocating clusters is a different categorisation process, with 21 clusters instead of several hundred diagnoses. Clustering does not use diagnosis because diagnosis is not well correlated with mental healthcare expenditure – other factors, such as marital status and electoral ward of residence, are better predictors of cost (Oyebode 2007).
The MHCT relies in large part on a set of scales developed by the Royal College of Psychiatrists’ Research Unit in the 1990s called the Health of the Nation Outcome Scales (HoNOS) (Wing 1996), so it does have clinical credentials, but
there is no scheme to translate backwards and forwards between diagnosis and clustering. A person with a diagnosis of first-episode psychosis could be allocated to one of several clusters, such as ‘psychotic crisis’, ‘first-episode psychosis’ or
‘ongoing or recurrent psychosis (high symptom and disability)’. A person with a cluster allocation of ‘psychotic crisis’ may have a clinical diagnosis of schizophrenia, mania, depression or personality disorder. The cluster is a single price that
covers all psychiatric comorbidities in a single category. A person with multiple psychiatric diagnoses (e.g. depression, substance misuse and personality disorder) will only receive one mental health cluster.
Gaming
Financial incentives change behaviour. The behaviour that organisations and individuals engage in to maximise income is sometimes called gaming. General practitioner commissioners have complained that trusts in acute physical care game their PbR systems. Gaming can create perverse activity. For example, some trusts facing financial penalties for failing to meet 4-hour waiting time targets in accident and emergency (A & E) departments apparently made patients wait outside in ambulances so as to delay the actual entry to A & E, when the clock starts ticking.
Up-coding
Financial gaming is limited with block budgets that are remote from clinicians, but mental healthcare practitioners using PbR will be immersed in the financial process. With PbR, each patient has a regular financial assessment by a clinician, who assigns a price to the patient. Practitioners usually want to get the best service for their patients and may tweak their clustering tool ratings up a bit to achieve a higher-paying cluster. This will be easy to do as they become familiar with the idiosyncrasies of the clustering algorithm. As a result, clinicians might assign more patients to high-value clusters (this is called up-coding and increases income without increasing quality). It is likely that internal and external audit processes (another cost) will be needed to monitor systematic up- or down-coding.
Cream-skimming and dumping
Service providers may decide to reorganise their services to include only simple, predictable cases that bring in a steady income (sometimes called cream-skimming), leaving patients with more complex needs (and higher financial risks) with
less input (dumping).
Combatting gaming
Organisational and clinical entrepreneurs will use the PbR system to their advantage, so it is very important that there are clear measures of patient benefit and harm to make sure that patients do not lose out. Some of these measures need to be independent of the MHCT, since gaming of the tool for income necessarily would game the outcome derived from HoNOS. Up-coding on initial assessment both increases income and inflates future positive outcomes, so there is a double incentive to exaggerate cluster assignments. Although CROMs have value, it may be the PROMs and PREMs that are the most independent and transparent.
Summary
Mental health PbR and clustering constitute a highly disruptive financial mechanism for funding mental healthcare that brings the NHS closer to a market approach. There are still many challenges ahead and it is quite possible that mental health PbR may not work out. The purchaser/provider split is not a panacea for service improvement, and
state-funded services can increase efficiency and quality without it (Timmins 2013).
Implementation has been put back more than once, but mental health PbR still appears to be on the way and services need to be prepared. Clustering will reduce clinical time for patients, but the impact can be lessened with good IT support and good training. Gaming will be easy and should be discouraged from the outset by emphasising probity and professionalism. Outcome measures will be introduced and these could help patients and practitioners understand what kind of care really works.
New providers, including big business and the voluntary sector, can enter the market. Small independent providers and individuals could benefit because they may be able to access money currently bound up in block contracts. There
will also be losers in a market approach. Among service providers, the losers could be those that do not upgrade their IT systems and those that fail to engage and train their staff. Many clinicians just want to get on with their primary jobs. For
them, the best approach to clustering is to try to do it accurately and quickly. The Care Pathways & Packages Project (CPPP) is developing the clustering currency.
Payment by results for mental health services: economic considerations of case-mix funding
Rowena Jacobs
Advances in psychiatric treatment (2014), vol. 20, 155–164
Summary
Against the backdrop of a tight financial climate, a new method of funding mental health services is being rolled out in England’s National Health Service. Called payment by results (PbR), it represents a fundamental change to the way providers of psychiatric services are paid for care of patients. The Mental Health Clustering Tool has been developed to capture activity which reflects the relative needs of patients, and cluster costs are being collected by service providers. The ultimate goal is the creation of a national tariff or fixed price for each cluster. This article describes the incentives generated by PbR and gives evidence on PbR in acute physical care services where it has been in operation for a decade, with respect to efficiency, quality, volume of activity, administrative costs, upcoding or gaming, equity of provision, and cross-subsidisation. It explores the challenges for mental health services as PbR is introduced.
Learning objectives
• Understand the difference between retrospective and prospective reimbursement systems and the incentives generated by each financing system.
• Understand the three key building blocks of PbR: currency, reference costs and tariffs.
• Consider the evidence on PbR in acute physical care and the implications for mental health services.
Healthcare financing and incentives
Retrospective reimbursement
At present, NHS mental health services are primarily funded through block contracts agreed between commissioners and providers of care, or on the basis of levels of existing ‘inputs’ such as the number of beds. This method of financing, often termed retrospective reimbursement, offers little incentive for providers to deliver an efficient level of care because it does not encourage them to control costs or increase output (activity levels). This is because an agreed fixed sum is paid regardless of the number of patients treated. Budgets are typically notionally fixed and renegotiated on the basis of past expenditure.
Retrospective payment typically allows the provider to receive funding for each day of care, each diagnostic test, or each procedure which is conducted (e.g. fee for service) and the full cost of each patient is therefore shifted to the payer (e.g. the insurer or the state). There is a clear link for the provider between their revenue and the use of resources per case. Under retrospective reimbursement, the payer refunds the actual costs incurred by each provider, which shifts risk to the payer.
Prospective reimbursement : payment by results
An alternative method of finance is when the price the provider is paid is set prospectively. The price paid per unit of healthcare activity is fixed in advance, giving an incentive for the provider to control their unit costs and increase the amount of service and activity levels provided, with a view to generating provider efficiency savings. PbR is a prospective payment system which was introduced into the English NHS in 2003–2004, beginning with acute healthcare providers.
Under prospective payment, the provider receives a lump-sum payment or fixed price which is set equal to the national average cost for patients with a particular condition or undergoing a particular procedure. This is often termed case-mix or activity-based funding and the lump-sum payment is set on the basis of case-mix- and resource homogeneous groupings called diagnosis-related groups (DRGs) or the NHS variant, healthcare resource groups (HRGs). These should classify patients into a grouping with an approximately similar case mix, who should consume an approximately similar amount of treatment resources (e.g. bed days, staff time, theatre time).
Implementation of PbR in the acute sector
Payment by results, the prospective payment system in England (Department of Health 2002), has run for a decade in acute physical care and was introduced to achieve three objectives, to:
Currency, costing and tariffs
The three key building blocks of PbR are a currency, reference costs and tariffs.
Currency
The currency is the nationally agreed unit of activity attracting payment. It can take a number of forms covering different time periods, from an out-patient attendance or a stay in hospital (e.g. an HRG) to a year of care for a long-term condition, or in the case of mental health, a care cluster.
Care clusters
Importantly, mental health services have taken a very different approach to currency development based on the Mental Health Clustering Tool (MHCT), which generates 21 case-mix clusters. The MHCT is based on the 12 items comprising
the Health of the Nation Outcome Scales (HoNOS) (Wing 1996) and 6 additional items comprising the Summary of Assessments of Risk and Need (SARN) (Self 2008). The MHCT does not use ICD-10 codes, but is based on the characteristics and needs of the patient. Consequently, patients with the same diagnosis could be assigned to
different clusters. Considerable variation within and between clusters in terms of case mix may therefore be evident.
Research is still required to establish the reliability, validity, and case-mix and resource homogeneity of the proposed clusters, as there is little independent research in support of their use.
Evidence from a national data assurance audit found that 40% of the clusters audited had at least one error. The main reasons for errors were: failure to follow MHCT guidance; poor quality of the medical records used to justify cluster decisions; and inaccurate recording of the dates that patients start care, change clusters or are discharged. Thus, continued efforts should be made to train and retrain clinical teams in the effective use of the MHCT, and regular audit of the process is needed.
Reference costs
The reference costs are a schedule each provider submits to the Department of Health detailing how much it costs them to provide each unit of the currency. Reference costs for mental health services have been collected by cluster since
2010–2011. Costs are collected for three types of activity: admitted (in-patient) and non-admitted (out-patient) care, and initial assessments. Reference costs are collected from NHS providers only. Private providers do not submit such costs, even though PbR applies to them when they provide care for NHS patients. A large proportion of mental health
activity is carried out by private providers and their cost structures may look very different from those of the NHS (e.g. contributions to employees’ pension schemes).
The tariff is based on the national average of all NHS provider reference costs for a given currency, which is then turned into the prospective national fixed price. Whether the public and private sectors should face the same tariffs is a matter of some debate, but in England a uniform tariff is set for provision for NHS patients. The maximum review period for
each of the 21 mental health clusters (determining when reassessments should occur), the indicative cluster unit costs and cluster costs per review period, and the number of patients in each cluster. As expected, the unit costs per cluster increase as illness severity and patient need increase for particular conditions. Commissioners will pay providers monthly for each patient in each cluster. Although mental health services do not yet have a fixed tariff, these costs provide an indication of the data that will be used and the method that will be applied to generate the tariff.
Tariff
The tariff, which has been delayed, will be calculated annually as a weighted average of admitted and non-admitted care and initial assessments. The clusters are designed to be independent of setting, thus providing an incentive to treat people in the least restrictive but also the most cost-effective setting. This strengthens incentives
to shape care pathways and to keep patients out of hospital, since providers will only be able to make a surplus if they minimise the more expensive inpatient costs relative to treating more patients in an out-patient setting.
Acute services had a decade of collecting and refining their costing processes before tariffs were introduced. For mental health the timescales of moving towards a national tariff have been considerably shorter and this may ultimately prove to be unwise with respect to the implementation of PbR. To date, there is evidence of very wide variation in costs at cluster level both within and across providers (Healthcare Financial Management Association 2012), suggesting that validation of the costing processes and consideration of the appropriateness of the clusters for costing purposes are required. There will inevitably be variation in data quality due to variations in provider efficiency, differences in service delivery models, the quality of services, the level of local authority input, as well as historical and procedural factors. There is also significant variation between providers in information technology (IT) systems, which adds complexity. Very few mental health providers, compared with acute providers, underpin the costing data with patient level information costing systems (PLICS) (PriceWaterhouseCoopers 2012), which can generate more detailed information on cost drivers and provide an important understanding of the relationship between cost and price. Setting prices on the basis of poor-quality cost data could significantly compromise PbR.
Summary
Before implementation in mental health services, it is essential that the three key building blocks of PbR (currency, reference costs and tariff) are thoroughly tested and that they are scrutinised by evaluators who are independent of the architects of the system. If the objective is to create a reimbursement system that incentivises implementation of national policy and strategies such as the Mental Health Strategy (Department of Health 2011a), and it is important that the system generates the right incentives for quality and service improvement alongside delivering efficiency improvements, then a thorough evaluation of the impact of PbR in mental health is needed.
What about quality?
It should be noted that ‘payment by results’ is something of a misnomer. Aside from a few initiatives such as best-practice tariffs (BPTs) to incentivise quality, payment is only for activity and does not take into account the undeniably important and rapidly developing area of routine outcome measurement in healthcare.
Work has been ongoing in mental healthcare to develop a range of quality indicators and outcome measures which can be used alongside the currency model to eventually enable payment linked to quality and outcomes (Department of Health 2011b). The intention is for clusters to be associated with quality and outcome measures:
• a set of quality indicators (e.g. the percentage of people on the care programme approach who have had an annual review; the percentage of patients with a valid ICD-10 diagnosis recorded; the completeness of ethnicity recording)
• clinician-rated outcome measures (CROMs) (based on HoNOS individual items and total scores using a four-factor model developed to show overall change and change specific to personal, emotional and social well-being and severe disturbance (Speak 2012))
• patient-reported outcome measures (PROMs) (e.g. the Warwick–Edinburgh Mental Well-being Scale)
• patient-reported experience measures (PREMs) (e.g. use of a ‘friends and family’ question); PREMs are likely to be derived from the Care Quality Commission’s (CQC’s) patient survey questions (Department of Health 2013).
Upcoding
In mental health services, the incentives for something akin to ‘cluster creep’ are more direct. Scoring for the MHCT is performed by members of the clinical team rather than clinical coders. With only 21 clusters, it will soon become apparent to clinical teams what the monetary value is for each. There is a computerised algorithm to support decision-making, but this can still be manually overridden. Small changes to the HoNOS item score profiles will map through to the MHCT. Patients could be moved between clusters to directly influence provider revenue and the moves could be disguised as variations in clinical judgement. There will therefore need to be checks in place to audit the mechanics of the clustering process and the integrity of this coding pathway. This will be very difficult to perform routinely and with neutral impact, since it raises suspicion while aiming to remove deception, and commissioners will not readily be in a position to audit upcoding at individual patient level. A continual validation of the algorithm for the MHCT will also be needed to ensure a consistent grouping of patients with similar needs.
Conclusions
Advocates for the PbR approach suggest that it has the capacity to reform and improve public services by delivering more for less and rewarding only what works. Indeed, some of the evidence would appear to support this view, although a significant challenge remains how to determine what constitutes the ‘result’ for which services will be paid.
A report by the King’s Fund questioned whether PbR is fit for purpose given changing priorities such as the need for the development of integrated care, the prevalence of long-term conditions and the changing economic environment. Among the key findings of the report was that:
• PbR is most suited to elective care and less suited to other services and that different services may require different payment systems
• the development of more comprehensive payments is needed
• the payment system needs to be underpinned by good information and analysis.
In January 2013, at a King’s Fund conference entitled ‘Payment Reform: Moving Beyond Payment by Results’, Emma Stanton, chief executive of Beacon UK, noted that while the acute sector is considering life beyond PbR, mental health services are still striving to adopt the PbR approach. Yet in many respects, mental health is already ahead of the curve on some aspects of PbR compared with acute physical care.
First, mental health is already grappling with the challenge of incorporating quality metrics, including CROMs, PROMs and PREMs, into the clusters to transform ‘payment by activity’ into something potentially better, but technically more challenging, i.e. ‘payment by results’.
Second, mental health is considering a more comprehensive payment approach essentially by using, as a currency, care clusters that encompass a patient’s complete care pathway. So, for example, ‘severe psychotic depression’
captures the full care pathway, as opposed to, say, ‘major hip procedures category 2 for trauma with intermediate complications’, which will have separate payments for out-patient follow-up appointments or rehabilitation and thus does not
incentivise joined-up care.
Yet for mental health the broader currency of case-mix clusters that encompass complete care pathways brings with it the problem of accurately costing such clusters, which will by design incorporate great variability in service elements. The establishing of accurate, reliable and meaningful cost data may become one of the biggest impediments to the implementation of PbR in mental healthcare.
An important part of the new payment system will be good information and robust and replicable analysis that includes the capturing of clustering decisions and their costs, as well as patientreported outcomes and quality metrics in the Mental Health Minimum Dataset (MHMDS). An evaluation is needed of the chosen currency, costs and resource implications, particularly in terms of the degree of variation within and between clusters and providers with respect to need, typical care pathways and case mix. This is challenging because diagnostic information in the MHMDS is currently poorly recorded by many providers. Gathering evidence through research and evaluation to support PbR
development is endorsed by the custodians of the future system (NHS England 2013). Although there are significant challenges in making the new system work in mental health services and some risks associated with doing so, an even greater risk is to do nothing. Furthermore, this is not an option: progress has begun. Mental health services that remain under block contracts risk disinvestment relative to services that have made it easier for commissioners to assess what they are spending their limited budgets on, particularly in the current financial climate.
Rowena Jacobs
Advances in psychiatric treatment (2014), vol. 20, 155–164
Summary
Against the backdrop of a tight financial climate, a new method of funding mental health services is being rolled out in England’s National Health Service. Called payment by results (PbR), it represents a fundamental change to the way providers of psychiatric services are paid for care of patients. The Mental Health Clustering Tool has been developed to capture activity which reflects the relative needs of patients, and cluster costs are being collected by service providers. The ultimate goal is the creation of a national tariff or fixed price for each cluster. This article describes the incentives generated by PbR and gives evidence on PbR in acute physical care services where it has been in operation for a decade, with respect to efficiency, quality, volume of activity, administrative costs, upcoding or gaming, equity of provision, and cross-subsidisation. It explores the challenges for mental health services as PbR is introduced.
Learning objectives
• Understand the difference between retrospective and prospective reimbursement systems and the incentives generated by each financing system.
• Understand the three key building blocks of PbR: currency, reference costs and tariffs.
• Consider the evidence on PbR in acute physical care and the implications for mental health services.
Healthcare financing and incentives
Retrospective reimbursement
At present, NHS mental health services are primarily funded through block contracts agreed between commissioners and providers of care, or on the basis of levels of existing ‘inputs’ such as the number of beds. This method of financing, often termed retrospective reimbursement, offers little incentive for providers to deliver an efficient level of care because it does not encourage them to control costs or increase output (activity levels). This is because an agreed fixed sum is paid regardless of the number of patients treated. Budgets are typically notionally fixed and renegotiated on the basis of past expenditure.
Retrospective payment typically allows the provider to receive funding for each day of care, each diagnostic test, or each procedure which is conducted (e.g. fee for service) and the full cost of each patient is therefore shifted to the payer (e.g. the insurer or the state). There is a clear link for the provider between their revenue and the use of resources per case. Under retrospective reimbursement, the payer refunds the actual costs incurred by each provider, which shifts risk to the payer.
Prospective reimbursement : payment by results
An alternative method of finance is when the price the provider is paid is set prospectively. The price paid per unit of healthcare activity is fixed in advance, giving an incentive for the provider to control their unit costs and increase the amount of service and activity levels provided, with a view to generating provider efficiency savings. PbR is a prospective payment system which was introduced into the English NHS in 2003–2004, beginning with acute healthcare providers.
Under prospective payment, the provider receives a lump-sum payment or fixed price which is set equal to the national average cost for patients with a particular condition or undergoing a particular procedure. This is often termed case-mix or activity-based funding and the lump-sum payment is set on the basis of case-mix- and resource homogeneous groupings called diagnosis-related groups (DRGs) or the NHS variant, healthcare resource groups (HRGs). These should classify patients into a grouping with an approximately similar case mix, who should consume an approximately similar amount of treatment resources (e.g. bed days, staff time, theatre time).
Implementation of PbR in the acute sector
Payment by results, the prospective payment system in England (Department of Health 2002), has run for a decade in acute physical care and was introduced to achieve three objectives, to:
- ‘enable […] commissioners to focus on the quality and volume of services provided’ (a fixed price would negate the need for price negotiations between commissioners and providers)
- ‘incentivise NHS Trusts to manage costs efficiently’ (providers would have the incentive to retain surpluses and increase the volume of activity)
- ‘create greater transparency and planning certainty in the system’ (when combined with other concurrent English healthcare reforms such as patient choice, these objectives would be realised because the money would follow the patient).
Currency, costing and tariffs
The three key building blocks of PbR are a currency, reference costs and tariffs.
Currency
The currency is the nationally agreed unit of activity attracting payment. It can take a number of forms covering different time periods, from an out-patient attendance or a stay in hospital (e.g. an HRG) to a year of care for a long-term condition, or in the case of mental health, a care cluster.
Care clusters
Importantly, mental health services have taken a very different approach to currency development based on the Mental Health Clustering Tool (MHCT), which generates 21 case-mix clusters. The MHCT is based on the 12 items comprising
the Health of the Nation Outcome Scales (HoNOS) (Wing 1996) and 6 additional items comprising the Summary of Assessments of Risk and Need (SARN) (Self 2008). The MHCT does not use ICD-10 codes, but is based on the characteristics and needs of the patient. Consequently, patients with the same diagnosis could be assigned to
different clusters. Considerable variation within and between clusters in terms of case mix may therefore be evident.
Research is still required to establish the reliability, validity, and case-mix and resource homogeneity of the proposed clusters, as there is little independent research in support of their use.
Evidence from a national data assurance audit found that 40% of the clusters audited had at least one error. The main reasons for errors were: failure to follow MHCT guidance; poor quality of the medical records used to justify cluster decisions; and inaccurate recording of the dates that patients start care, change clusters or are discharged. Thus, continued efforts should be made to train and retrain clinical teams in the effective use of the MHCT, and regular audit of the process is needed.
Reference costs
The reference costs are a schedule each provider submits to the Department of Health detailing how much it costs them to provide each unit of the currency. Reference costs for mental health services have been collected by cluster since
2010–2011. Costs are collected for three types of activity: admitted (in-patient) and non-admitted (out-patient) care, and initial assessments. Reference costs are collected from NHS providers only. Private providers do not submit such costs, even though PbR applies to them when they provide care for NHS patients. A large proportion of mental health
activity is carried out by private providers and their cost structures may look very different from those of the NHS (e.g. contributions to employees’ pension schemes).
The tariff is based on the national average of all NHS provider reference costs for a given currency, which is then turned into the prospective national fixed price. Whether the public and private sectors should face the same tariffs is a matter of some debate, but in England a uniform tariff is set for provision for NHS patients. The maximum review period for
each of the 21 mental health clusters (determining when reassessments should occur), the indicative cluster unit costs and cluster costs per review period, and the number of patients in each cluster. As expected, the unit costs per cluster increase as illness severity and patient need increase for particular conditions. Commissioners will pay providers monthly for each patient in each cluster. Although mental health services do not yet have a fixed tariff, these costs provide an indication of the data that will be used and the method that will be applied to generate the tariff.
Tariff
The tariff, which has been delayed, will be calculated annually as a weighted average of admitted and non-admitted care and initial assessments. The clusters are designed to be independent of setting, thus providing an incentive to treat people in the least restrictive but also the most cost-effective setting. This strengthens incentives
to shape care pathways and to keep patients out of hospital, since providers will only be able to make a surplus if they minimise the more expensive inpatient costs relative to treating more patients in an out-patient setting.
Acute services had a decade of collecting and refining their costing processes before tariffs were introduced. For mental health the timescales of moving towards a national tariff have been considerably shorter and this may ultimately prove to be unwise with respect to the implementation of PbR. To date, there is evidence of very wide variation in costs at cluster level both within and across providers (Healthcare Financial Management Association 2012), suggesting that validation of the costing processes and consideration of the appropriateness of the clusters for costing purposes are required. There will inevitably be variation in data quality due to variations in provider efficiency, differences in service delivery models, the quality of services, the level of local authority input, as well as historical and procedural factors. There is also significant variation between providers in information technology (IT) systems, which adds complexity. Very few mental health providers, compared with acute providers, underpin the costing data with patient level information costing systems (PLICS) (PriceWaterhouseCoopers 2012), which can generate more detailed information on cost drivers and provide an important understanding of the relationship between cost and price. Setting prices on the basis of poor-quality cost data could significantly compromise PbR.
Summary
Before implementation in mental health services, it is essential that the three key building blocks of PbR (currency, reference costs and tariff) are thoroughly tested and that they are scrutinised by evaluators who are independent of the architects of the system. If the objective is to create a reimbursement system that incentivises implementation of national policy and strategies such as the Mental Health Strategy (Department of Health 2011a), and it is important that the system generates the right incentives for quality and service improvement alongside delivering efficiency improvements, then a thorough evaluation of the impact of PbR in mental health is needed.
What about quality?
It should be noted that ‘payment by results’ is something of a misnomer. Aside from a few initiatives such as best-practice tariffs (BPTs) to incentivise quality, payment is only for activity and does not take into account the undeniably important and rapidly developing area of routine outcome measurement in healthcare.
Work has been ongoing in mental healthcare to develop a range of quality indicators and outcome measures which can be used alongside the currency model to eventually enable payment linked to quality and outcomes (Department of Health 2011b). The intention is for clusters to be associated with quality and outcome measures:
• a set of quality indicators (e.g. the percentage of people on the care programme approach who have had an annual review; the percentage of patients with a valid ICD-10 diagnosis recorded; the completeness of ethnicity recording)
• clinician-rated outcome measures (CROMs) (based on HoNOS individual items and total scores using a four-factor model developed to show overall change and change specific to personal, emotional and social well-being and severe disturbance (Speak 2012))
• patient-reported outcome measures (PROMs) (e.g. the Warwick–Edinburgh Mental Well-being Scale)
• patient-reported experience measures (PREMs) (e.g. use of a ‘friends and family’ question); PREMs are likely to be derived from the Care Quality Commission’s (CQC’s) patient survey questions (Department of Health 2013).
Upcoding
In mental health services, the incentives for something akin to ‘cluster creep’ are more direct. Scoring for the MHCT is performed by members of the clinical team rather than clinical coders. With only 21 clusters, it will soon become apparent to clinical teams what the monetary value is for each. There is a computerised algorithm to support decision-making, but this can still be manually overridden. Small changes to the HoNOS item score profiles will map through to the MHCT. Patients could be moved between clusters to directly influence provider revenue and the moves could be disguised as variations in clinical judgement. There will therefore need to be checks in place to audit the mechanics of the clustering process and the integrity of this coding pathway. This will be very difficult to perform routinely and with neutral impact, since it raises suspicion while aiming to remove deception, and commissioners will not readily be in a position to audit upcoding at individual patient level. A continual validation of the algorithm for the MHCT will also be needed to ensure a consistent grouping of patients with similar needs.
Conclusions
Advocates for the PbR approach suggest that it has the capacity to reform and improve public services by delivering more for less and rewarding only what works. Indeed, some of the evidence would appear to support this view, although a significant challenge remains how to determine what constitutes the ‘result’ for which services will be paid.
A report by the King’s Fund questioned whether PbR is fit for purpose given changing priorities such as the need for the development of integrated care, the prevalence of long-term conditions and the changing economic environment. Among the key findings of the report was that:
• PbR is most suited to elective care and less suited to other services and that different services may require different payment systems
• the development of more comprehensive payments is needed
• the payment system needs to be underpinned by good information and analysis.
In January 2013, at a King’s Fund conference entitled ‘Payment Reform: Moving Beyond Payment by Results’, Emma Stanton, chief executive of Beacon UK, noted that while the acute sector is considering life beyond PbR, mental health services are still striving to adopt the PbR approach. Yet in many respects, mental health is already ahead of the curve on some aspects of PbR compared with acute physical care.
First, mental health is already grappling with the challenge of incorporating quality metrics, including CROMs, PROMs and PREMs, into the clusters to transform ‘payment by activity’ into something potentially better, but technically more challenging, i.e. ‘payment by results’.
Second, mental health is considering a more comprehensive payment approach essentially by using, as a currency, care clusters that encompass a patient’s complete care pathway. So, for example, ‘severe psychotic depression’
captures the full care pathway, as opposed to, say, ‘major hip procedures category 2 for trauma with intermediate complications’, which will have separate payments for out-patient follow-up appointments or rehabilitation and thus does not
incentivise joined-up care.
Yet for mental health the broader currency of case-mix clusters that encompass complete care pathways brings with it the problem of accurately costing such clusters, which will by design incorporate great variability in service elements. The establishing of accurate, reliable and meaningful cost data may become one of the biggest impediments to the implementation of PbR in mental healthcare.
An important part of the new payment system will be good information and robust and replicable analysis that includes the capturing of clustering decisions and their costs, as well as patientreported outcomes and quality metrics in the Mental Health Minimum Dataset (MHMDS). An evaluation is needed of the chosen currency, costs and resource implications, particularly in terms of the degree of variation within and between clusters and providers with respect to need, typical care pathways and case mix. This is challenging because diagnostic information in the MHMDS is currently poorly recorded by many providers. Gathering evidence through research and evaluation to support PbR
development is endorsed by the custodians of the future system (NHS England 2013). Although there are significant challenges in making the new system work in mental health services and some risks associated with doing so, an even greater risk is to do nothing. Furthermore, this is not an option: progress has begun. Mental health services that remain under block contracts risk disinvestment relative to services that have made it easier for commissioners to assess what they are spending their limited budgets on, particularly in the current financial climate.
Measuring the Activity of Mental Health Services in England: Variation in Categorising Activity for Payment Purposes
Rowena Jacobs, Martin Chalkley, Jan R. Böhnke, Michael Clark, Valerie Moran, M. J. Aragón
Administration and Policy in Mental Health and Mental Health Services Research (2019) 46:847–857
Published online: 27 July 2019
Discussion
Contribution to the Current Evidence Base This paper has explored the proposed episodic payment approach for mental health services in England whereby clinicians allocate patients into one of 21 clusters on the basis of similar levels of need using the MHCT. For this episodic payment system to work effectively, there should not be too much variation in costs or resource use either within clusters, or between providers. We tested whether the existing unit of activity, namely clusters, which underpin the collection of mental health activity and cost data amongst English mental health providers,
would support the new payment system. Specifically, we examined the variation both within clusters and between mental health providers in terms of their costs and activity/resource use.
We contribute to the evidence base by examining the implementation of care clusters as a unit of activity in mental health, with a key need being more robust analysis of cluster data. Our results suggest a large amount of variation between providers in terms of costs, activity rates and length of stay within clusters. There is substantial variability between providers in the length of cluster episodes, and there is huge variability within clusters in terms of the proportion of inpatient days and the proportion of contact with health care professionals. We find longer cluster episodes do not translate into proportionally more activity in terms of either inpatient days or contacts with health care professionals. With high levels of variation within clusters, accurate baseline activity rates cannot be determined for planning and purchasing care. Variation in activity rates means that providers see different numbers of patients, have different treatment approaches, levels of productivity, and put different care pathways and packages of care in place for patients within each cluster. This could lead to differences in care quality and outcomes across providers, generating potential geographic inequalities for patients. While the average costs per cluster broadly correspond to severity as indicated by the cluster labels, there is also enormous variation within clusters in terms of costs. Variations in cost mean that patients with similar levels of need may be using different levels of resource, leading to a potential waste of scarce resources or an under-treatment of some people in some localities. This also suggests that the introduction of an episodic payment approach would result in large variation across providers in terms of their financial positions.
Our findings of significant heterogeneity in costs, and significant heterogeneity in terms of resource use, do not bode well for an episodic payment approach which requires resource homogeneity within clusters. The reduction of variation in care, activity levels and costs is pivotal to the establishment of a well-designed classification and payment system.
Of course, some of the variation we have found could be a result of data quality issues, including poor costing systems, poor coding, and differing allocation of patients to clusters between individual clinicians and providers. Even if this is the case, it still does not augur well for an episodic payment system since until the data quality issues are resolved, the analysis underpinning it will result in inappropriate payments to providers.
Rowena Jacobs, Martin Chalkley, Jan R. Böhnke, Michael Clark, Valerie Moran, M. J. Aragón
Administration and Policy in Mental Health and Mental Health Services Research (2019) 46:847–857
Published online: 27 July 2019
Discussion
Contribution to the Current Evidence Base This paper has explored the proposed episodic payment approach for mental health services in England whereby clinicians allocate patients into one of 21 clusters on the basis of similar levels of need using the MHCT. For this episodic payment system to work effectively, there should not be too much variation in costs or resource use either within clusters, or between providers. We tested whether the existing unit of activity, namely clusters, which underpin the collection of mental health activity and cost data amongst English mental health providers,
would support the new payment system. Specifically, we examined the variation both within clusters and between mental health providers in terms of their costs and activity/resource use.
We contribute to the evidence base by examining the implementation of care clusters as a unit of activity in mental health, with a key need being more robust analysis of cluster data. Our results suggest a large amount of variation between providers in terms of costs, activity rates and length of stay within clusters. There is substantial variability between providers in the length of cluster episodes, and there is huge variability within clusters in terms of the proportion of inpatient days and the proportion of contact with health care professionals. We find longer cluster episodes do not translate into proportionally more activity in terms of either inpatient days or contacts with health care professionals. With high levels of variation within clusters, accurate baseline activity rates cannot be determined for planning and purchasing care. Variation in activity rates means that providers see different numbers of patients, have different treatment approaches, levels of productivity, and put different care pathways and packages of care in place for patients within each cluster. This could lead to differences in care quality and outcomes across providers, generating potential geographic inequalities for patients. While the average costs per cluster broadly correspond to severity as indicated by the cluster labels, there is also enormous variation within clusters in terms of costs. Variations in cost mean that patients with similar levels of need may be using different levels of resource, leading to a potential waste of scarce resources or an under-treatment of some people in some localities. This also suggests that the introduction of an episodic payment approach would result in large variation across providers in terms of their financial positions.
Our findings of significant heterogeneity in costs, and significant heterogeneity in terms of resource use, do not bode well for an episodic payment approach which requires resource homogeneity within clusters. The reduction of variation in care, activity levels and costs is pivotal to the establishment of a well-designed classification and payment system.
Of course, some of the variation we have found could be a result of data quality issues, including poor costing systems, poor coding, and differing allocation of patients to clusters between individual clinicians and providers. Even if this is the case, it still does not augur well for an episodic payment system since until the data quality issues are resolved, the analysis underpinning it will result in inappropriate payments to providers.
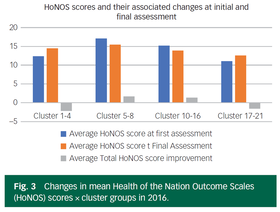
Desperately seeking outcomes: quantifying the effectiveness of community mental healthcare using Health of the Nation Outcome Scales
Richard Laugharne, Scott Eaves, Alin Mascas, Kiki Psatha, Gill Dinnis, Jonathan Trower and Rohit Shankar
BJPsych Open (2018)
Background
Community mental health services in the UK have struggled to measure the clinical effectiveness of their services.
Aims
To measure clinical outcomes for different diagnostic clusters.
Method
Clinicians measure the clinical status of patients by the Health of the Nation Outcome Scales (HoNOS), and HoNOS scores should be recorded annually after treatment. Clinical outcomes were measured by changes in HoNOS for diagnostic clusters.
Results
In two time periods (2014 and 2016), the health of patients with mild to moderate common mental disorders deteriorated after intervention. Patients with severe common mental disorders and psychoses improved in their clinical status.
Discussion
The data demonstrate that CMHTs tend to perform better for patients with severe and complex non-psychotic and psychotic disorders. It is not surprising that patients with cognitive impairment do not tend to see an improvement following intervention from CMHTs according to HoNOS score as dementia is a progressive illness. The worsening HoNOS scores in this group gives validity to the use of the average total score.
It is surprising that HoNOS has not been used for outcome data but rather as a clustering tool in England. Mental health services have struggled to establish outcome measures for their service and have focused on process measures instead. We need to use outcome measures to establish which services are effective in improving people’s lives. This can help drive the investment in useful mental health services when we are effectively competing for funds with other areas of medicine that can clearly demonstrate clinical benefit.
Although HoNOS has limitations in validity and reliability, we believe there are opportunities to use changes in total HoNOS scores to demonstrate service effectiveness and performance at all levels, from the individual patient to the team and Trust. At the moment it is the best outcome measure we have as it has been used for nearly a decade.
Our data suggest that CMHT input is effective for patients with severe and enduring mental illnesses (clusters 5–16), which is good news. However our results suggest that for mild to moderate mental illness, CMHT input is not effective. This strengthens the case for having clear boundaries in referring those patients to counselling/primary care talking therapies.
Richard Laugharne, Scott Eaves, Alin Mascas, Kiki Psatha, Gill Dinnis, Jonathan Trower and Rohit Shankar
BJPsych Open (2018)
Background
Community mental health services in the UK have struggled to measure the clinical effectiveness of their services.
Aims
To measure clinical outcomes for different diagnostic clusters.
Method
Clinicians measure the clinical status of patients by the Health of the Nation Outcome Scales (HoNOS), and HoNOS scores should be recorded annually after treatment. Clinical outcomes were measured by changes in HoNOS for diagnostic clusters.
Results
In two time periods (2014 and 2016), the health of patients with mild to moderate common mental disorders deteriorated after intervention. Patients with severe common mental disorders and psychoses improved in their clinical status.
Discussion
The data demonstrate that CMHTs tend to perform better for patients with severe and complex non-psychotic and psychotic disorders. It is not surprising that patients with cognitive impairment do not tend to see an improvement following intervention from CMHTs according to HoNOS score as dementia is a progressive illness. The worsening HoNOS scores in this group gives validity to the use of the average total score.
It is surprising that HoNOS has not been used for outcome data but rather as a clustering tool in England. Mental health services have struggled to establish outcome measures for their service and have focused on process measures instead. We need to use outcome measures to establish which services are effective in improving people’s lives. This can help drive the investment in useful mental health services when we are effectively competing for funds with other areas of medicine that can clearly demonstrate clinical benefit.
Although HoNOS has limitations in validity and reliability, we believe there are opportunities to use changes in total HoNOS scores to demonstrate service effectiveness and performance at all levels, from the individual patient to the team and Trust. At the moment it is the best outcome measure we have as it has been used for nearly a decade.
Our data suggest that CMHT input is effective for patients with severe and enduring mental illnesses (clusters 5–16), which is good news. However our results suggest that for mild to moderate mental illness, CMHT input is not effective. This strengthens the case for having clear boundaries in referring those patients to counselling/primary care talking therapies.
MODELS FOR PAYING PROVIDERS OF NHS SERVICES
To help you understand the different ways in which providers can be paid for seeing and treating patients, including block contracts, capitation, the national tariff and payment for performance.
The British Medical Association (BMA) is the trade union and professional body for doctors in the UK.
UK, Tuesday 6 July 2021
https://www.bma.org.uk/advice-and-support/nhs-delivery-and-workforce/funding/models-for-paying-providers-of-nhs-services
Block contracts have been widely used throughout the UK, and continue to be the main payment system for hospitals in Scotland, Wales and Northern Ireland.
In England, the national tariff (payment by results) currently dominates payments made to the acute sector.
New, integrated models of care mean that other ways to pay providers may become more dominant.
Block contracts
A block contract is a payment made to a provider to deliver a specific, usually broadly-defined, service. For example, a hospital could be given a block contract to undertake acute care in a particular area.
How the value of a block contract is calculated varies widely. It can be set through a measure of patient need or it may be based on the historical spend of a particular service.
Pros
Capitation
Capitation is a payment system where lump-sum payments are made to care providers based on the number of patients in a target population, to provide some or all of their care needs. The capitation payment is not linked to how much care is provided.
Capitation is used to determine core funding for UK general practice. However, most sustainability and transformation plans in England also aim to move towards an outcome-based capitated budget.
Pros
The national tariff
The national tariff currently dominates payments made to the acute sector in England. HRGs (health resource groups) are used to determine the pricing for health care services.
The national tariff currently dominates payments made to the acute sector in England. HRGs are used to determine the pricing for health care services.
DRGs/HRGs are not used in the NHS in Scotland, Northern Ireland or Wales, where block contracts remain the dominant payment system.
Pros
Payment for performance
Payment-for-performance schemes refer to payment arrangements where providers are financially rewarded for achieving high performance or quality. Each scheme rewards providers in a unique way.
In primary care, the QOF (quality and outcomes framework) rewards GP practices for achieving performance indicators.
Scotland is considering new payment arrangements to QOF for GP practices and Wales has agreed reforms going forward.
Quality metrics or indicators can be broken down into three categories:
The BMA's view
The BMA does not support the national tariff, payment by results, as the main way for paying acute providers in England.
Instead we would prefer to see a new payment model introduced that encourages closer working between different parts of the health service, around the needs of patients.
Current payment reforms that focus on capitation look, at present, to be the most realistic way of achieving these aims.
New models for delivering care - Payment models for integrated care - A capitated payment approach
bma-payment-models-for-integrated-care-2017.pdf
Background
The main payment system in England, the national tariff, is widely recognised as posing a barrier to integration. Some areas are already moving towards other payment systems, such as block contracts or outcomes-based contracts, to facilitate integration. NHS Improvement and NHS England are also working with some areas to develop a new payment approach, which may be adopted by emerging MCPs (multispecialty community providers), PACS (primary and acute care systems). This briefing focuses on the approach they are developing, which is based on capitation. See our other briefings for further information on existing payment models (eg the national tariff), and MCPs and PACS.
A capitated payment approach
Capitation is a payment system where lump-sum payments are made to care providers based on the number of patients in a population, to provide some or all of their care needs. It is not linked to how much care is provided. Capitation is currently used to determine core general practice funding. A capitated, whole population budget forms the basis of the new payment approach, along with an improvement payment scheme and a gain/loss share arrangement. Together, these elements are intended to enable longer-term planning and a more flexible use of resources to best meet the needs of the whole population, with targeted financial incentives.
Implementation
NHS Improvement and NHS England have been working with MCPs, PACS and other sites to develop this approach. A number of sites have begun to test elements of the model, although it is unlikely that any will go fully live until April 2018. Some practicalities are still being worked through, such as how to disaggregate existing block contracts (commonly used in community care and mental health services). Initial guidance on the payment approach has been published, and will be followed by a more comprehensive ‘handbook’.2 In time, it is likely to become part of the national tariff process; however, for now it remains a voluntary approach and may be subject to further refinement.
What’s the BMA’s policy?
The BMA has been and remains clear that the current payment system in England (the national tariff) is not fit for purpose and does not support integrated working around the needs of patients. Following a literature review in 2015 (before the detail of the new capitated payment approach had been developed), we concluded that: ‘payment reforms that focus on capitation look, at present, to be the most realistic way of achieving closer working between different parts of the health service’. It is essential that any capitated budget is sufficient to fund services and accommodate local variations (eg in population health). However, the assumption behind many new care models, that shifting care out of hospital will save money, is not supported by evidence. Any movement of care into the community must be adequately funded. The financial challenges facing the NHS are well-documented and the risk of taking on responsibility and accountability for a whole population budget must not be underestimated. This is particularly pertinent for GP partners and practices operating as providers as part of an MCP. We believe spending for core general practice should be ring-fenced, to ensure these essential services are protected for all patients, regardless of postcode. We also have concerns that a single capitated budget could result in unintended consequences, such as a pressure to reduce referral rates, particularly where there is a need to run an overall profit to provide adequate income or meet internal fiscal targets. This not only risks patient care, but risks doctors’ professional duty and relationship with patients. Targets for outcomes or activity levels in any gain/loss share arrangement must be carefully considered, as service demand (particularly for A&E) can be very difficult to predict or control. Improving patient care must be the priority and complexity within the system, should be minimised where possible.
To help you understand the different ways in which providers can be paid for seeing and treating patients, including block contracts, capitation, the national tariff and payment for performance.
The British Medical Association (BMA) is the trade union and professional body for doctors in the UK.
UK, Tuesday 6 July 2021
https://www.bma.org.uk/advice-and-support/nhs-delivery-and-workforce/funding/models-for-paying-providers-of-nhs-services
Block contracts have been widely used throughout the UK, and continue to be the main payment system for hospitals in Scotland, Wales and Northern Ireland.
In England, the national tariff (payment by results) currently dominates payments made to the acute sector.
New, integrated models of care mean that other ways to pay providers may become more dominant.
Block contracts
A block contract is a payment made to a provider to deliver a specific, usually broadly-defined, service. For example, a hospital could be given a block contract to undertake acute care in a particular area.
How the value of a block contract is calculated varies widely. It can be set through a measure of patient need or it may be based on the historical spend of a particular service.
Pros
- They are timely, predictable and relatively flexible.
- Payments are made on a regular, usually annual, basis.
- Some commissioners and providers favour block contracts because of the low transaction costs.
- Often used where other payment methods would not be financially viable because of low activity levels or budgetary constraints.
- Lack of transparency and accountability after a payment has been made to a provider.
- As block contracts are made in advance of a service being delivered, unexpected pressures such as increased patient demand or cost of care are not taken into account.
- They do not incentivise improved clinical care or efficiency.
Capitation
Capitation is a payment system where lump-sum payments are made to care providers based on the number of patients in a target population, to provide some or all of their care needs. The capitation payment is not linked to how much care is provided.
Capitation is used to determine core funding for UK general practice. However, most sustainability and transformation plans in England also aim to move towards an outcome-based capitated budget.
Pros
- As a capitated payment is not linked to how much care is provided, providers have the flexibility to spend money on services they think will secure the best outcome for the patient.
- The potential for more integrated care and evidence that professionals work more closely together when working under a capitated budget.
- Evaluations of programmes elsewhere show they are more cost-effective than other payment systems.
- Providers are paid regardless of what they deliver - enabling them to provide as little care as possible to minimise costs.
- They do not necessarily take in to account changes in levels of demand, as has been seen in general practice.
- Services delivered by different organisations require significant capabilities on the provider side - eg coordination between primary and secondary care and sophisticated IT to track individual patients' activities.
The national tariff
The national tariff currently dominates payments made to the acute sector in England. HRGs (health resource groups) are used to determine the pricing for health care services.
The national tariff currently dominates payments made to the acute sector in England. HRGs are used to determine the pricing for health care services.
DRGs/HRGs are not used in the NHS in Scotland, Northern Ireland or Wales, where block contracts remain the dominant payment system.
Pros
- As providers are paid according to levels of activity, it encourages them to treat more patients, which can lead to reduced waiting times.
- Increased efficiency and system-wide cost containment - HRG-based payment systems are calculated using average costs and so this encourages those hospitals with above average costs to become more efficient.
- Potential for providers to skimp on quality in order to reduce their costs and maximise profit.
- ‘Cream skimming’ where providers seek out healthier and/or lower-risk patients, or focus on certain conditions or procedures.
- Despite the inclusion of some best practice tariffs and the CQUIN (commissioning for quality and innovation’ framework), the connection between the national tariff and patient outcomes remains poor.
- It does not facilitate a more coordinated approach to health care delivery, across other sectors or parts of the NHS.
Payment for performance
Payment-for-performance schemes refer to payment arrangements where providers are financially rewarded for achieving high performance or quality. Each scheme rewards providers in a unique way.
In primary care, the QOF (quality and outcomes framework) rewards GP practices for achieving performance indicators.
Scotland is considering new payment arrangements to QOF for GP practices and Wales has agreed reforms going forward.
Quality metrics or indicators can be broken down into three categories:
- patient outcomes (such as mortality and readmission rates)
- process measures (such as waiting times and screening rates)
- clinical process measures (such as measuring blood pressure).
- There is evidence that payment-for-performance schemes can lead to a clinically-significant reduction in mortality rates.
- Can lead to improvements in quality in terms of process and clinical process measures.
- They are not guaranteed to improve patient outcomes and other quality measures.
- When financial incentives are used to influence performance, leading to a so-called ‘tick box’ culture, those rewards can undermine performance and worsen motivation.
- Can divert attention from other, unrewarded activities.
- Unlikely that they will save money overall.
The BMA's view
The BMA does not support the national tariff, payment by results, as the main way for paying acute providers in England.
Instead we would prefer to see a new payment model introduced that encourages closer working between different parts of the health service, around the needs of patients.
Current payment reforms that focus on capitation look, at present, to be the most realistic way of achieving these aims.
New models for delivering care - Payment models for integrated care - A capitated payment approach
bma-payment-models-for-integrated-care-2017.pdf
Background
The main payment system in England, the national tariff, is widely recognised as posing a barrier to integration. Some areas are already moving towards other payment systems, such as block contracts or outcomes-based contracts, to facilitate integration. NHS Improvement and NHS England are also working with some areas to develop a new payment approach, which may be adopted by emerging MCPs (multispecialty community providers), PACS (primary and acute care systems). This briefing focuses on the approach they are developing, which is based on capitation. See our other briefings for further information on existing payment models (eg the national tariff), and MCPs and PACS.
A capitated payment approach
Capitation is a payment system where lump-sum payments are made to care providers based on the number of patients in a population, to provide some or all of their care needs. It is not linked to how much care is provided. Capitation is currently used to determine core general practice funding. A capitated, whole population budget forms the basis of the new payment approach, along with an improvement payment scheme and a gain/loss share arrangement. Together, these elements are intended to enable longer-term planning and a more flexible use of resources to best meet the needs of the whole population, with targeted financial incentives.
Implementation
NHS Improvement and NHS England have been working with MCPs, PACS and other sites to develop this approach. A number of sites have begun to test elements of the model, although it is unlikely that any will go fully live until April 2018. Some practicalities are still being worked through, such as how to disaggregate existing block contracts (commonly used in community care and mental health services). Initial guidance on the payment approach has been published, and will be followed by a more comprehensive ‘handbook’.2 In time, it is likely to become part of the national tariff process; however, for now it remains a voluntary approach and may be subject to further refinement.
What’s the BMA’s policy?
The BMA has been and remains clear that the current payment system in England (the national tariff) is not fit for purpose and does not support integrated working around the needs of patients. Following a literature review in 2015 (before the detail of the new capitated payment approach had been developed), we concluded that: ‘payment reforms that focus on capitation look, at present, to be the most realistic way of achieving closer working between different parts of the health service’. It is essential that any capitated budget is sufficient to fund services and accommodate local variations (eg in population health). However, the assumption behind many new care models, that shifting care out of hospital will save money, is not supported by evidence. Any movement of care into the community must be adequately funded. The financial challenges facing the NHS are well-documented and the risk of taking on responsibility and accountability for a whole population budget must not be underestimated. This is particularly pertinent for GP partners and practices operating as providers as part of an MCP. We believe spending for core general practice should be ring-fenced, to ensure these essential services are protected for all patients, regardless of postcode. We also have concerns that a single capitated budget could result in unintended consequences, such as a pressure to reduce referral rates, particularly where there is a need to run an overall profit to provide adequate income or meet internal fiscal targets. This not only risks patient care, but risks doctors’ professional duty and relationship with patients. Targets for outcomes or activity levels in any gain/loss share arrangement must be carefully considered, as service demand (particularly for A&E) can be very difficult to predict or control. Improving patient care must be the priority and complexity within the system, should be minimised where possible.
The NHS payment system: evolving policy and emerging evidence
Nuffield Trust - Research report
Louise Marshall, Anita Charlesworth, Jeremy Hurst
February 2014
www.nuffieldtrust.org.uk/publications/nhs-payment-system-policy
Approaches to paying for health care
The system used to pay for health care encompasses both the unit of service for which payment is made (the currency) and the price paid for that service. Many factors can be varied in the design of a payment system for health care, and the optimal design will depend on the objectives of the health care system. For instance, payments can be made to the provider to:
• cover a range of services for a specified time period (block budget)
• care for a specific patient or population (capitation)
• provide specific services (fee-for-service)
• provide a specified quality of processes or outcomes of care (performance-related pay).
Payments to providers may be made prospectively as a fixed amount, based on assessment of local patient needs and prediction of services needed by the population served. In these cases, agreements will be needed between commissioners and providers as to where the risk and benefit fall if actual provision is above or below the predicted level. Alternatively, payment may be retrospective, reimbursing providers for actual services provided following the event; in this case, there may be an upper limit on the amount of service that will be paid for. Payments for a service may be directly proportional to the units of that service or may be conditional on reaching a threshold or target level, and the unit payment may change based on volume. The level of payment may be fixed or subject to negotiation between commissioners and providers, and may also vary depending on the characteristics of the provider or the patient seen. Payments may be withheld or reduced for non-compliance.
Payment methods in health care
The main payment methods in health care can be ordered by the extent to which they ‘bundle’ together payments for services. At one end of this spectrum are block budgets; at the other, fee-for-service payments.
Block budgets
The payment for all services to be provided is bundled together, and a prospective lump sum is paid to a provider at defined intervals, independent of the number of patients treated or the amount of activity undertaken. A block budget provides an overall spending limit that will constrain the volume and/or quality of the services provided. Under this arrangement, the provider bears the risk for increased demand and cost of care, and the commissioner for decreases, unless there are
arrangements to share risk or surplus. The ability of a block budget to achieve policy objectives will be dependent on contractual conditions of the payment (for example, around quality, efficiency and volume) and also on the proportion of the provider’s total revenue included in the block. Salary payments, in which the periodic lump sum for bundled services provided is paid to an individual, are similar to block budgets.
Advantages:
• Transaction costs are low.
• Expenditure/income is predictable if the budget has a fixed cap and no further payment can be made for additional costs incurred by the provider.
• Provides flexibility for provider innovation – where this is cost-neutral or cost-reducing – as providers can change the service without it having a direct impact on their income.
Disadvantages:
• Lacks transparency and accountability.
• Increases in activity are disincentivised.
• Cost-increasing breakthrough innovation is disincentivised; added to this is the constrained access that providers have to capital finance, and flexibility to innovate where up-front investment is required, is limited.
• Excess demand may cause providers to ration services or result in a decline in the quality of care, without additional mechanisms to sustain volume or quality, or improve efficiency.
• Providers may avoid or under-serve costly, high-need and complex patients.
• Choice and competition are not supported as money does not follow the patient.
• ‘Better’ providers will attract more work, but not more resources; conversely, providers performing less well may attract fewer patients, but would not lose resources.
Capitation
Prospective, periodic, lump-sum payments are made to a provider or a network of providers per enrolled patient, for a range of bundled, specified services. Ideally, capitated budgets are ‘weighted’ (risk-adjusted) to take account of the fact that some
patients require additional, or more costly, services.
Advantages:
• Transaction costs are low, although weighting adds cost.
• Cost containment and financial control are supported.
• Providers are incentivised to attract more patients as money follows the patient, which may in principle incentivise improved quality in dimensions of care that patients value and can observe.
Disadvantages:
• There is no incentive to provide additional or more costly services for patients enrolled.
• If there is no patient choice of provider, capitation funding provides no incentive for providers to be responsive to patients. In fact, it can create an incentive for providers to discourage patient utilisation by being unresponsive.
• If payments are not fully risk-adjusted, providers may avoid patients with high levels of need, or those whose needs are under-compensated for by the weighting formula.
• If the capitation payment covers only part of the patient’s health care (for example, primary care), there is an incentive for providers to shift more care to other services and limit the range of care they provide.
• While in principle providers have some incentive to invest in prevention, this is rarely the case in practice. Single-year contracts are not sufficiently long for potential savings from preventive interventions to be realised by providers; hence investment in these is not encouraged, and providers have stronger incentives to save costs by lowering quantity or quality of services. Contracts either do not adequately specify or enforce minimum standards, and additional payment mechanisms are increasingly being used alongside capitated contracts to incentivise high-priority preventive interventions.
Case-based payments
Providers are paid a fixed sum for an episode of care, based on groupings of clinically similar diagnoses or procedures that entail similar costs. This method involves less bundling than capitation payments, as reimbursement is for an episode of care, rather than a period which may or may not include activity. Some bundling remains, however, as an episode may include multiple activities. Similarly, payments may be made for a defined pathway of care, for a patient with a particular diagnosis. Risk is apportioned between commissioners and providers: in principle, ‘epidemiological’ risk (arising from
variations in the incidence of disease) falls on the commissioner; while ‘clinical’ risk (associated with what is done to the patient) falls on the provider. However, this distinction can break down in the presence of supplier-induced demand or billable readmissions caused by avoidable errors in care or complications.
Advantages:
• Patient choice and competition are supported as money follows episodes of care.
• Improvements to quality may be incentivised through patient choice.
• Grouping episodes by diagnosis can facilitate comparisons of clinical quality to inform choice and also facilitates benchmarking of costs.
• Providers are incentivised to reduce cost per episode (an advantage only if this is achieved through productivity improvements rather than a decline in quality).
• Increases in activity are incentivised (only an advantage if this is cost-effective and appropriate activity, for instance to reduce waiting times).
Disadvantages:
• The incentive to treat more patients might stimulate unwanted as well as desired activity through ‘supplier-induced demand’.
• Financial control for commissioners is more difficult, unless a limit on volume is specified.
• Transaction costs are higher due to the need for billing and more sophisticated costing systems.
• Quality may fall as a result of attempts to increase profit by reducing costs of care where prices are fixed.
• Providers may be disincentivised to introduce quality-raising but cost-increasing new technologies.
• Providers may select the least complicated patients, who are likely to cost less to treat.
• Providers may ‘up-code’ classification of patients into a more highly reimbursed group.
• Service innovation may be more difficult as currency and payment levels reflect past models of care and costs.
Fee-for-service
Payment is made retrospectively to providers for each unit of service provided, in other words, each activity or patient contact, according to a fixed price schedule. All the risk for increasing cost falls on the commissioner.
Advantages:
• Supports patient choice and competition, and thereby possibly increases in quality.
• Could promote equity of care, as providers are paid for all treatment they choose to provide.
• Supports quality and comprehensive care as the provider has no incentive to withhold or skimp on care.
• Rapidly supports innovation that expands or changes the use of treatments and technologies already on the reimbursement list, which can be reimbursed quickly.
Disadvantages:
• Highly challenging to financial control and likely to increase spending through increases in activity as a result of supplier-led demand, or through their specific treatment decisions.
• Providers are not incentivised to improve efficiency or to work jointly with other providers.
• Providers are not incentivised to prevent future ill health, unless preventive interventions are specifically paid for, with a sufficiently attractive margin. Moreover, there is no incentive to take a population-level approach to prevention.
• Can delay innovations that require addition of a new technology to the reimbursement list, as control of entry to the list is a mechanism for control of expenditure under fee-for-service.
While payment systems are important levers for influencing provider behaviour, as discussed above, there are disadvantages and risks associated with all approaches, some of which may act as a barrier to achievement of health care objectives. Balancing and mitigating these to achieve the desired signals is highly complex. To add to the complexity, the payment system is just one among multiple incentive tools and other factors that influence provider behaviour. These can act synergistically with the payment system, or may contradict and negate signals provided through payment. It is therefore
important that different priorities and levers are aligned.
Key considerations when designing pay-for-performance schemes
• The definition of ‘performance’ and whether to link payments to absolute or relative levels. Plus, if the latter, whether this is comparative between providers, or related to change within a provider over time.
• The ability to measure the aspects of performance that are of importance. Delivery of health care requires multiple actions, some of which can be observed and measured and others not/less well. Rewarding performance first requires the ability
to measure it.
• Selection of performance targets in areas with known room for improvement, as the impact and hence the value for money may be insignificant in areas where extensive quality improvement work has recently been undertaken.
• The problem of attention shift. There is the risk that unmeasured/unrewarded work may be sacrificed for measured/rewarded work, which could have negative consequences for overall efficiency and patient outcomes. This is particularly concerning where pay-for-performance targets are determined by what can be measured, rather than what is of direct importance.
• Pay-for-performance frequently rewards compliance with processes of care, rather than outcomes. This is largely because processes are easier to measure and outcomes often distant in time and difficult to attribute to a single activity. In this way, pay-for-performance can become equivalent to fee-for-service.
• If rewards are based on outcomes, however, and only partial adjustments can be made for patient characteristics, providers may avoid treating sicker patients or those with complex conditions.
• Extrinsic motivation provided by incentive schemes can reduce intrinsic motivation, which is generally high among health professionals.
• Pay-for-performance may act as a barrier to creativity and innovation by increasing the financial risk associated with these, and thereby can encourage practice by rote.
Review of evidence from evaluation of NHS payment programmes
Secondary care: mental health and community services
While almost two thirds of hospital activity is covered by activity-based payment, through the national tariff, the predominant payment system for the remaining secondary care services has been the block budget, with block contracts used to reimburse around 90 per cent of community services, and two thirds of mental health care. Local tariffs reimburse the remainder of these services.
A mental health currency was published in 2010/11, which proposed that contracting for mental health services should utilise bundled, period payments (care clusters) for 20 specified conditions, for durations of between four weeks and a year (Department of Health, 2011a). The clusters were created during 2012/13, and providers asked to define packages of care associated with these. Tariffs will be based on costs of these packages, as submitted by providers. Although the intention was to introduce the tariff during 2013/14, the Department of Health recognises that this is too soon, but is asking commissioners and providers to prepare (Department of Health, 2012c). In 2013/14, CCGs and providers should agree a local price for each cluster. Currencies are also being developed for a wider range of mental health services including the Improved Access to Psychological Therapies (IAPT) service and Child and Adolescent Mental Health Services (CAHMS) (Monitor and NHS England, 2013b).
The other key group of services not covered by a tariff payment system is community health services. Community health services are diverse in function and differ widely between localities across England. They include a wide range of services based outside hospitals, including care for long-term chronic conditions, preventive services, and assessment and rehabilitation services; plus community hospital services, some non-acute inpatient hospital care, and hospice care.
Although there has been discussion about national community service tariffs, progress has been slow, hindered by local diversity of services, and lack of uniform activity and costing data (Department of Health, 2008). Attempts have been made to extend the patient choice agenda to mental health and community services. In 2011, local areas identified at least three (of a list of eight) services in which they would implement the ‘Any Qualified Provider’ scheme in 2012/13 (Department of Health, 2011b). This allows patients to choose from a selection of commissioned providers when referred by their GP. Competition between ‘qualified’ providers is on the basis of quality, rather than price, with all providers being paid a fixed price (NHS Supply2Health). While the national tariff sets this price for elective hospital care, commissioners will set prices locally for mental health and community services in line with guidelines from the Department of Health. Pay-for-performance aspects are added to the payment system for mental health and community services through CQUIN schemes. In 2014/15, further quality and outcomes measurement is planned for mental health services, and Monitor proposes that payments to providers could be varied according to the standards achieved for patients in the cluster. Mental
health provider payments will be activity-related and some element of patient choice is being introduced.
Taking a wider view
In summary, therefore, blended payment systems are common in the NHS. The GP contract combines elements of weighted capitation, pay-for-performance and fee-forservice. For hospitals, diagnosis-related payments coexist with block budgets, retrospective per-day payments for certain outlier patients with unexpectedly long lengths of stay, and some fee-for-service for, for example, unbundled diagnostics. However, while the balance of methods within health sectors has been subject to attention and reform over the last decade, the balance across sectors is also important.
Taking a wider view of the payment system for the overall NHS budget will be an important step in developing the optimal balance of spending across services to both meet the needs of the population and maximise the cost-efficiency of provision. In doing this, it must be borne in mind that the payment approach that is most effective in achieving higher-quality care and better value is likely to vary according to the context of care.
Activity-based payment approaches such as Payment by Results work best in contexts where:
• the episode of care has a well-defined start and finish point
• the care is planned in advance
• there is evidence demonstrating the benefit and cost-effectiveness of the care to the patient.
They are helpful where priorities are enabling choice for patients, increasing productivity, and increasing utilisation of particular services, or by target population groups (where the criteria for payment must be well defined to address identified inequalities in access). As priorities differ across contexts, so will the optimal method, and the design of the NHS payment system needs to be flexible to accommodate a range of approaches that can be applied to different contexts (Monitor and NHS England, 2013a).
There has been far more development to payment for acute services than for community and mental health. Perhaps partly as a consequence of this, cost, quality and outcomes data are poorly developed for these services. In turn, this is a limitation to the development of payment systems, and must be urgently addressed to tackle imbalances across the system and barriers to policy ambitions to shift care.
Currently, the predominance of activity-based payment for acute and emergency care in theory incentivises increased activity in this sector. In parallel, the predominance of block budgets for community services and capitation for primary care services could disincentivise increased activity. Given the policy ambition to shift care out of hospital
and closer to the home, this imbalance must be addressed to prevent the incentives acting as a barrier. Neither do block budgets promote productivity improvements. If care is to be shifted into the community, productivity improvements will be needed to manage increased activity, given current budgetary limitations.
Recent local and national developments have included attempts to design payment systems that can apply across services and that support shifting of care. A number of examples involve bundling of service payments to include capitation-based ‘year of care’ payments for life-long conditions such as cystic fibrosis and for high-risk, multimorbidity patients (Monitor and NHS England, 2013a), and pathway-based payments for maternity services. Another approach being explored is unbundling of payments. As part of the drive to shift care out of hospitals, the ‘recovery, rehabilitation and reablement’ (RRR) model separates the current acute tariff into the acute care phase and the postacute RRR phase, allowing this to be commissioned in the community rather than hospital, where appropriate (Department of Health, 2012e). These approaches are, however, still experimental and evaluations will in future provide invaluable evidence as to the feasibility of these sorts of approaches.
Summary
The payment system is a lever to support the delivery of high-quality, cost-effective care, but it is only one lever among multiple available to commissioners. It is imperative that the limitations of a payment approach are recognised in the objectives set for it, which should be based on what good evidence tells us payment approaches may be able to achieve. The objectives that have been set for the redesigned payment system for NHS care are highly ambitious. There are intentions that it will reimburse outcomes, support changing patterns of care and better links between health and wider sectors, as well as enable the efficient allocation of resources. These are perhaps overly ambitious in light of what evidence tells us the payment approaches can achieve.
The evidence presented in this report supports a role for financial incentives in improving the quality and productivity of processes of care. However, there is a lack of evidence for an impact on patient outcomes. It is important therefore that a distinction is made between primary objectives for the payment system, based on robust evidence for an effect, and those factors that the payment system should enable and support. Based on the research, primary objectives supported by evidence are as follows:
• to incentivise improvements in quality
• to incentivise improvements in efficiency and productivity
• to ensure resources are allocated both appropriately and efficiently, following the patient and matching need rather than demand
• to ensure transparency and accountability for the use of public resources.
In addition to these primary objectives, the payment system must enable and support other aims of the health service. There is a lack of evidence for a primary role of payment in directly incentivising these, and non-payment approaches may be more effective in achieving changes in these other areas. At the very least, it must be ensured that the payment system is not acting as a barrier to achieving change in these areas, through unintended consequences of approaches taken. These wider ambitions of the health service that the payment system must support include:
• achievement of outcomes
• better integration and coordination of services both within and between sectors
• patient choice
• innovation, both in health care and health care payment systems.
What is clear from the evidence is that better data, better use of data, and better evaluation of payment systems must be priorities. Until this can be made a reality, there is a case for caution regarding what payment reform can achieve. The most important opportunities in the short to medium term are around ensuring that the payment system allocates resources efficiently and does not create perverse incentives or undermine the other policy levers that can influence outcomes for patients. This urgently requires better activity and cost data across sectors, particularly in community, mental health and
primary care services. Without this, cross-system goals will not be possible.
The roles of local and central bodies also must be defined. While local identification of goals is beneficial in many ways, there is a key role for central bodies in providing resources for coding, pricing and indicator setting where replication of these tasks at local level would consume too many resources or create confusing variation.
Nuffield Trust - Research report
Louise Marshall, Anita Charlesworth, Jeremy Hurst
February 2014
www.nuffieldtrust.org.uk/publications/nhs-payment-system-policy
Approaches to paying for health care
The system used to pay for health care encompasses both the unit of service for which payment is made (the currency) and the price paid for that service. Many factors can be varied in the design of a payment system for health care, and the optimal design will depend on the objectives of the health care system. For instance, payments can be made to the provider to:
• cover a range of services for a specified time period (block budget)
• care for a specific patient or population (capitation)
• provide specific services (fee-for-service)
• provide a specified quality of processes or outcomes of care (performance-related pay).
Payments to providers may be made prospectively as a fixed amount, based on assessment of local patient needs and prediction of services needed by the population served. In these cases, agreements will be needed between commissioners and providers as to where the risk and benefit fall if actual provision is above or below the predicted level. Alternatively, payment may be retrospective, reimbursing providers for actual services provided following the event; in this case, there may be an upper limit on the amount of service that will be paid for. Payments for a service may be directly proportional to the units of that service or may be conditional on reaching a threshold or target level, and the unit payment may change based on volume. The level of payment may be fixed or subject to negotiation between commissioners and providers, and may also vary depending on the characteristics of the provider or the patient seen. Payments may be withheld or reduced for non-compliance.
Payment methods in health care
The main payment methods in health care can be ordered by the extent to which they ‘bundle’ together payments for services. At one end of this spectrum are block budgets; at the other, fee-for-service payments.
Block budgets
The payment for all services to be provided is bundled together, and a prospective lump sum is paid to a provider at defined intervals, independent of the number of patients treated or the amount of activity undertaken. A block budget provides an overall spending limit that will constrain the volume and/or quality of the services provided. Under this arrangement, the provider bears the risk for increased demand and cost of care, and the commissioner for decreases, unless there are
arrangements to share risk or surplus. The ability of a block budget to achieve policy objectives will be dependent on contractual conditions of the payment (for example, around quality, efficiency and volume) and also on the proportion of the provider’s total revenue included in the block. Salary payments, in which the periodic lump sum for bundled services provided is paid to an individual, are similar to block budgets.
Advantages:
• Transaction costs are low.
• Expenditure/income is predictable if the budget has a fixed cap and no further payment can be made for additional costs incurred by the provider.
• Provides flexibility for provider innovation – where this is cost-neutral or cost-reducing – as providers can change the service without it having a direct impact on their income.
Disadvantages:
• Lacks transparency and accountability.
• Increases in activity are disincentivised.
• Cost-increasing breakthrough innovation is disincentivised; added to this is the constrained access that providers have to capital finance, and flexibility to innovate where up-front investment is required, is limited.
• Excess demand may cause providers to ration services or result in a decline in the quality of care, without additional mechanisms to sustain volume or quality, or improve efficiency.
• Providers may avoid or under-serve costly, high-need and complex patients.
• Choice and competition are not supported as money does not follow the patient.
• ‘Better’ providers will attract more work, but not more resources; conversely, providers performing less well may attract fewer patients, but would not lose resources.
Capitation
Prospective, periodic, lump-sum payments are made to a provider or a network of providers per enrolled patient, for a range of bundled, specified services. Ideally, capitated budgets are ‘weighted’ (risk-adjusted) to take account of the fact that some
patients require additional, or more costly, services.
Advantages:
• Transaction costs are low, although weighting adds cost.
• Cost containment and financial control are supported.
• Providers are incentivised to attract more patients as money follows the patient, which may in principle incentivise improved quality in dimensions of care that patients value and can observe.
Disadvantages:
• There is no incentive to provide additional or more costly services for patients enrolled.
• If there is no patient choice of provider, capitation funding provides no incentive for providers to be responsive to patients. In fact, it can create an incentive for providers to discourage patient utilisation by being unresponsive.
• If payments are not fully risk-adjusted, providers may avoid patients with high levels of need, or those whose needs are under-compensated for by the weighting formula.
• If the capitation payment covers only part of the patient’s health care (for example, primary care), there is an incentive for providers to shift more care to other services and limit the range of care they provide.
• While in principle providers have some incentive to invest in prevention, this is rarely the case in practice. Single-year contracts are not sufficiently long for potential savings from preventive interventions to be realised by providers; hence investment in these is not encouraged, and providers have stronger incentives to save costs by lowering quantity or quality of services. Contracts either do not adequately specify or enforce minimum standards, and additional payment mechanisms are increasingly being used alongside capitated contracts to incentivise high-priority preventive interventions.
Case-based payments
Providers are paid a fixed sum for an episode of care, based on groupings of clinically similar diagnoses or procedures that entail similar costs. This method involves less bundling than capitation payments, as reimbursement is for an episode of care, rather than a period which may or may not include activity. Some bundling remains, however, as an episode may include multiple activities. Similarly, payments may be made for a defined pathway of care, for a patient with a particular diagnosis. Risk is apportioned between commissioners and providers: in principle, ‘epidemiological’ risk (arising from
variations in the incidence of disease) falls on the commissioner; while ‘clinical’ risk (associated with what is done to the patient) falls on the provider. However, this distinction can break down in the presence of supplier-induced demand or billable readmissions caused by avoidable errors in care or complications.
Advantages:
• Patient choice and competition are supported as money follows episodes of care.
• Improvements to quality may be incentivised through patient choice.
• Grouping episodes by diagnosis can facilitate comparisons of clinical quality to inform choice and also facilitates benchmarking of costs.
• Providers are incentivised to reduce cost per episode (an advantage only if this is achieved through productivity improvements rather than a decline in quality).
• Increases in activity are incentivised (only an advantage if this is cost-effective and appropriate activity, for instance to reduce waiting times).
Disadvantages:
• The incentive to treat more patients might stimulate unwanted as well as desired activity through ‘supplier-induced demand’.
• Financial control for commissioners is more difficult, unless a limit on volume is specified.
• Transaction costs are higher due to the need for billing and more sophisticated costing systems.
• Quality may fall as a result of attempts to increase profit by reducing costs of care where prices are fixed.
• Providers may be disincentivised to introduce quality-raising but cost-increasing new technologies.
• Providers may select the least complicated patients, who are likely to cost less to treat.
• Providers may ‘up-code’ classification of patients into a more highly reimbursed group.
• Service innovation may be more difficult as currency and payment levels reflect past models of care and costs.
Fee-for-service
Payment is made retrospectively to providers for each unit of service provided, in other words, each activity or patient contact, according to a fixed price schedule. All the risk for increasing cost falls on the commissioner.
Advantages:
• Supports patient choice and competition, and thereby possibly increases in quality.
• Could promote equity of care, as providers are paid for all treatment they choose to provide.
• Supports quality and comprehensive care as the provider has no incentive to withhold or skimp on care.
• Rapidly supports innovation that expands or changes the use of treatments and technologies already on the reimbursement list, which can be reimbursed quickly.
Disadvantages:
• Highly challenging to financial control and likely to increase spending through increases in activity as a result of supplier-led demand, or through their specific treatment decisions.
• Providers are not incentivised to improve efficiency or to work jointly with other providers.
• Providers are not incentivised to prevent future ill health, unless preventive interventions are specifically paid for, with a sufficiently attractive margin. Moreover, there is no incentive to take a population-level approach to prevention.
• Can delay innovations that require addition of a new technology to the reimbursement list, as control of entry to the list is a mechanism for control of expenditure under fee-for-service.
While payment systems are important levers for influencing provider behaviour, as discussed above, there are disadvantages and risks associated with all approaches, some of which may act as a barrier to achievement of health care objectives. Balancing and mitigating these to achieve the desired signals is highly complex. To add to the complexity, the payment system is just one among multiple incentive tools and other factors that influence provider behaviour. These can act synergistically with the payment system, or may contradict and negate signals provided through payment. It is therefore
important that different priorities and levers are aligned.
Key considerations when designing pay-for-performance schemes
• The definition of ‘performance’ and whether to link payments to absolute or relative levels. Plus, if the latter, whether this is comparative between providers, or related to change within a provider over time.
• The ability to measure the aspects of performance that are of importance. Delivery of health care requires multiple actions, some of which can be observed and measured and others not/less well. Rewarding performance first requires the ability
to measure it.
• Selection of performance targets in areas with known room for improvement, as the impact and hence the value for money may be insignificant in areas where extensive quality improvement work has recently been undertaken.
• The problem of attention shift. There is the risk that unmeasured/unrewarded work may be sacrificed for measured/rewarded work, which could have negative consequences for overall efficiency and patient outcomes. This is particularly concerning where pay-for-performance targets are determined by what can be measured, rather than what is of direct importance.
• Pay-for-performance frequently rewards compliance with processes of care, rather than outcomes. This is largely because processes are easier to measure and outcomes often distant in time and difficult to attribute to a single activity. In this way, pay-for-performance can become equivalent to fee-for-service.
• If rewards are based on outcomes, however, and only partial adjustments can be made for patient characteristics, providers may avoid treating sicker patients or those with complex conditions.
• Extrinsic motivation provided by incentive schemes can reduce intrinsic motivation, which is generally high among health professionals.
• Pay-for-performance may act as a barrier to creativity and innovation by increasing the financial risk associated with these, and thereby can encourage practice by rote.
Review of evidence from evaluation of NHS payment programmes
Secondary care: mental health and community services
While almost two thirds of hospital activity is covered by activity-based payment, through the national tariff, the predominant payment system for the remaining secondary care services has been the block budget, with block contracts used to reimburse around 90 per cent of community services, and two thirds of mental health care. Local tariffs reimburse the remainder of these services.
A mental health currency was published in 2010/11, which proposed that contracting for mental health services should utilise bundled, period payments (care clusters) for 20 specified conditions, for durations of between four weeks and a year (Department of Health, 2011a). The clusters were created during 2012/13, and providers asked to define packages of care associated with these. Tariffs will be based on costs of these packages, as submitted by providers. Although the intention was to introduce the tariff during 2013/14, the Department of Health recognises that this is too soon, but is asking commissioners and providers to prepare (Department of Health, 2012c). In 2013/14, CCGs and providers should agree a local price for each cluster. Currencies are also being developed for a wider range of mental health services including the Improved Access to Psychological Therapies (IAPT) service and Child and Adolescent Mental Health Services (CAHMS) (Monitor and NHS England, 2013b).
The other key group of services not covered by a tariff payment system is community health services. Community health services are diverse in function and differ widely between localities across England. They include a wide range of services based outside hospitals, including care for long-term chronic conditions, preventive services, and assessment and rehabilitation services; plus community hospital services, some non-acute inpatient hospital care, and hospice care.
Although there has been discussion about national community service tariffs, progress has been slow, hindered by local diversity of services, and lack of uniform activity and costing data (Department of Health, 2008). Attempts have been made to extend the patient choice agenda to mental health and community services. In 2011, local areas identified at least three (of a list of eight) services in which they would implement the ‘Any Qualified Provider’ scheme in 2012/13 (Department of Health, 2011b). This allows patients to choose from a selection of commissioned providers when referred by their GP. Competition between ‘qualified’ providers is on the basis of quality, rather than price, with all providers being paid a fixed price (NHS Supply2Health). While the national tariff sets this price for elective hospital care, commissioners will set prices locally for mental health and community services in line with guidelines from the Department of Health. Pay-for-performance aspects are added to the payment system for mental health and community services through CQUIN schemes. In 2014/15, further quality and outcomes measurement is planned for mental health services, and Monitor proposes that payments to providers could be varied according to the standards achieved for patients in the cluster. Mental
health provider payments will be activity-related and some element of patient choice is being introduced.
Taking a wider view
In summary, therefore, blended payment systems are common in the NHS. The GP contract combines elements of weighted capitation, pay-for-performance and fee-forservice. For hospitals, diagnosis-related payments coexist with block budgets, retrospective per-day payments for certain outlier patients with unexpectedly long lengths of stay, and some fee-for-service for, for example, unbundled diagnostics. However, while the balance of methods within health sectors has been subject to attention and reform over the last decade, the balance across sectors is also important.
Taking a wider view of the payment system for the overall NHS budget will be an important step in developing the optimal balance of spending across services to both meet the needs of the population and maximise the cost-efficiency of provision. In doing this, it must be borne in mind that the payment approach that is most effective in achieving higher-quality care and better value is likely to vary according to the context of care.
Activity-based payment approaches such as Payment by Results work best in contexts where:
• the episode of care has a well-defined start and finish point
• the care is planned in advance
• there is evidence demonstrating the benefit and cost-effectiveness of the care to the patient.
They are helpful where priorities are enabling choice for patients, increasing productivity, and increasing utilisation of particular services, or by target population groups (where the criteria for payment must be well defined to address identified inequalities in access). As priorities differ across contexts, so will the optimal method, and the design of the NHS payment system needs to be flexible to accommodate a range of approaches that can be applied to different contexts (Monitor and NHS England, 2013a).
There has been far more development to payment for acute services than for community and mental health. Perhaps partly as a consequence of this, cost, quality and outcomes data are poorly developed for these services. In turn, this is a limitation to the development of payment systems, and must be urgently addressed to tackle imbalances across the system and barriers to policy ambitions to shift care.
Currently, the predominance of activity-based payment for acute and emergency care in theory incentivises increased activity in this sector. In parallel, the predominance of block budgets for community services and capitation for primary care services could disincentivise increased activity. Given the policy ambition to shift care out of hospital
and closer to the home, this imbalance must be addressed to prevent the incentives acting as a barrier. Neither do block budgets promote productivity improvements. If care is to be shifted into the community, productivity improvements will be needed to manage increased activity, given current budgetary limitations.
Recent local and national developments have included attempts to design payment systems that can apply across services and that support shifting of care. A number of examples involve bundling of service payments to include capitation-based ‘year of care’ payments for life-long conditions such as cystic fibrosis and for high-risk, multimorbidity patients (Monitor and NHS England, 2013a), and pathway-based payments for maternity services. Another approach being explored is unbundling of payments. As part of the drive to shift care out of hospitals, the ‘recovery, rehabilitation and reablement’ (RRR) model separates the current acute tariff into the acute care phase and the postacute RRR phase, allowing this to be commissioned in the community rather than hospital, where appropriate (Department of Health, 2012e). These approaches are, however, still experimental and evaluations will in future provide invaluable evidence as to the feasibility of these sorts of approaches.
Summary
The payment system is a lever to support the delivery of high-quality, cost-effective care, but it is only one lever among multiple available to commissioners. It is imperative that the limitations of a payment approach are recognised in the objectives set for it, which should be based on what good evidence tells us payment approaches may be able to achieve. The objectives that have been set for the redesigned payment system for NHS care are highly ambitious. There are intentions that it will reimburse outcomes, support changing patterns of care and better links between health and wider sectors, as well as enable the efficient allocation of resources. These are perhaps overly ambitious in light of what evidence tells us the payment approaches can achieve.
The evidence presented in this report supports a role for financial incentives in improving the quality and productivity of processes of care. However, there is a lack of evidence for an impact on patient outcomes. It is important therefore that a distinction is made between primary objectives for the payment system, based on robust evidence for an effect, and those factors that the payment system should enable and support. Based on the research, primary objectives supported by evidence are as follows:
• to incentivise improvements in quality
• to incentivise improvements in efficiency and productivity
• to ensure resources are allocated both appropriately and efficiently, following the patient and matching need rather than demand
• to ensure transparency and accountability for the use of public resources.
In addition to these primary objectives, the payment system must enable and support other aims of the health service. There is a lack of evidence for a primary role of payment in directly incentivising these, and non-payment approaches may be more effective in achieving changes in these other areas. At the very least, it must be ensured that the payment system is not acting as a barrier to achieving change in these areas, through unintended consequences of approaches taken. These wider ambitions of the health service that the payment system must support include:
• achievement of outcomes
• better integration and coordination of services both within and between sectors
• patient choice
• innovation, both in health care and health care payment systems.
What is clear from the evidence is that better data, better use of data, and better evaluation of payment systems must be priorities. Until this can be made a reality, there is a case for caution regarding what payment reform can achieve. The most important opportunities in the short to medium term are around ensuring that the payment system allocates resources efficiently and does not create perverse incentives or undermine the other policy levers that can influence outcomes for patients. This urgently requires better activity and cost data across sectors, particularly in community, mental health and
primary care services. Without this, cross-system goals will not be possible.
The roles of local and central bodies also must be defined. While local identification of goals is beneficial in many ways, there is a key role for central bodies in providing resources for coding, pricing and indicator setting where replication of these tasks at local level would consume too many resources or create confusing variation.
Local payment examples - Mental healthcare: a capitated approach to payment with outcomes and risk share components
Local commissioners need to consider case by case how best to secure and pay for services that meet the needs of service users in their local area.
Local providers and commissioners looking to implement the payment approach described in this document while it is in its current development stage must follow the rules and principles for locally determined prices set out in Section 7.1 of the National Tariff Payment System. This includes a requirement to send to Monitor and publish any locally agreed payment arrangements that lead to changes to the national prices set by Monitor.
Commissioners and providers need to consider carefully how a payment approach based on services with local prices (such as mental health) could be used in the context of services with national prices (where a different local payment approach based on variation of national prices would be necessary). Where there is a mix of health and social care the national tariff rules continue to apply to the healthcare services.
Commissioners should also ensure that they follow the framework set out in the National Health Service (Procurement, Patient Choice and Competition) (No 2) Regulations 2013. Guidance by Monitor on these regulations is available here. Further background information on this local payment example and how it relates to other areas of Monitor’s work can be found here. www.gov.uk/government/collections/different.
https://www.gov.uk/search/all?keywords=payment+model&order=relevance
Commissioners and providers of mental healthcare need to place greater emphasis on achieving the right outcomes for service users. The use of agreed outcome measures in mental healthcare enables clinicians and providers to have a common vision of how to meet service user needs. It allows key units of measurement to move away from an emphasis on inputs, and offers a language to support care that is more patient-centred.
The inclusion of an outcomes-based component in payment approaches should incentivise providers and commissioners to provide and pay for services that promote better outcomes for patients, rather than better activities or processes. There is good evidence from national and international healthcare systems for a range of benefits to be gained from the inclusion of this component in payments.
Historically, mental healthcare has been paid for using block contracts and data flows have been centred on activity. This has not encouraged a detailed understanding of where and how service user needs are being met. Many providers and commissioners now use the mental healthcare clusters as the sole basis of payment: these group service users with similar care needs and relate payment to components such as a required number of appointments, attendances and specific treatments completed.
Outcomes-based payment draws the attention of all the players in a healthcare system to achieving the target patient outcomes because it rewards co-ordinated care arrangements that deliver those outcomes more efficiently. The approach is based on the assumption the efficiencies of the current healthcare system can be improved, as suggested by evidence from the United States, Valencia in Spain and many other areas. In these areas, payment arrangements combining a fixed core component based on capitation with an outcomes-based component have improved outcomes for service users and transformed the delivery of care (see Appendices 2 and 3 for examples). Evidence indicates that such payment arrangements offer benefits for patients, providers and local mental healthcare systems:
Benefits to patients:
o improved patient experience of care as this care is less fragmented and better co-ordinated
o improved outcomes, such as more time spent living independently at home, reduced acute readmissions and more timely access to care o better information for patients about their care o broader patient choice
Benefits to providers:
o more stable and predictable income, supporting service delivery
o better alignment of patient pathways and care processes with outcomes
o clearer definition from commissioners of what reimbursement will be based on, possibly for a period of several years
o development of a culture of collaboration and integration between providers across the mental health and social care economic system
Benefits to commissioners:
o binding contractual agreements with providers, with real rewards and penalties tied to defined outcomes and performance targets
o improved value for money shown by measurable benefits to patients
o streamlining of the bureaucracy and administration required to manage multiple providers and contracts
System-wide benefits:
o reduced duplication and transaction costs across organisations
o promotion of investment in prevention, quality improvement and working practices that deliver savings and efficiencies over the longer term, where contracts run for a sufficient length of time
o number of key performance indicators (KPIs) reduced to those central to improving patient outcomes.
Forms of contracting that can support co-ordinated approaches to outcomes-based payment
It is possible to link outcomes-based payment to almost any payment arrangement. It is also possible to arrange for service provision with a number of local providers through a range of co-ordinated contractual arrangements. These promote an outcomes-based payment approach that overtly shares common objectives across the system, including outcomes-based payment. Examples of such arrangements in England and elsewhere are:
Prime contractor: a single provider assumes all clinical and financial responsibility for delivering defined patient outcomes. This provider leads the integration of services for patients, sometimes along a whole care pathway, sometimes for a defined patient population, through subcontracts with other providers. Commissioners hold a single contract with the prime contractor. The prime contractor may be an existing provider, a broker or an integrating organisation.
Lead accountable provider: as above, a single provider is accountable for providing a whole care pathway or pathways, or achieving defined outcomes for a defined patient population. Commissioners hold a single contract with this provider, who may subcontract some parts of the pathway or some services. However, in this case, the lead accountable provider retains key accountability for delivery of appropriate, quality care on the pathway (see Section 5 for more details).
Alliance: typically led by commissioners, this contracting mechanism aims to incentivise a number of providers to co-operate to deliver a particular service or an interrelated set of services. Providers enter into linked contracts with commissioners, with the latter evaluating these collectively. Each party maintains its own internal financial controls and shares gain/loss risks with the other commissioners and providers in the alliance.
Joint venture: providers jointly create a new vehicle to facilitate provision of integrated care, but each provider remains independent. The joint venture agreement specifies its nature, responsibilities and governance. Commissioners contract with the joint venture (rather than individual providers) for the delivery of services.
Fully integrated care: as above, commissioners hold a single contract with a single direct or indirect provider of care, but this organisation assumes all responsibility for providing services for an entire care pathway or patient population.
Each of these delivery approaches has its own strengths and weaknesses, which are not explored fully in this document. However, when implementing any of them, commissioners and providers should take care to:
avoid double counting of services, ie ensure that services to be contracted to one or more providers are not contractually covered by another provider
include sufficient incentives in the contracts to encourage better co-ordination of services between all the providers involved; incentives should promote prevention, early intervention and treatment of service users in the lowest intensity care setting that is appropriate for their needs
develop service models capable of delivering co-ordinated services on a larger scale, as well as the mechanisms for recording and sharing the data necessary for managing the delivery of larger, longer-term contracts and monitoring progress on outcomes.
The lead accountable provider model
In this model, commissioners have a single contract with one provider organisation – the lead provider – which may have one of two broad types of accountability.
For a defined population: a lead provider or group of providers is accountable for managing an agreed range of health and social care needs and achieving agreed outcomes for a defined population. The contract may apply to the care for a local population within a specific geography or to the care for a clearly defined segment of this population.
For a defined pathway: the provider(s) is accountable for service user outcomes from the commissioned single ‘pathway’ of care for a particular condition over a defined period of time.
Local commissioners need to consider case by case how best to secure and pay for services that meet the needs of service users in their local area.
Local providers and commissioners looking to implement the payment approach described in this document while it is in its current development stage must follow the rules and principles for locally determined prices set out in Section 7.1 of the National Tariff Payment System. This includes a requirement to send to Monitor and publish any locally agreed payment arrangements that lead to changes to the national prices set by Monitor.
Commissioners and providers need to consider carefully how a payment approach based on services with local prices (such as mental health) could be used in the context of services with national prices (where a different local payment approach based on variation of national prices would be necessary). Where there is a mix of health and social care the national tariff rules continue to apply to the healthcare services.
Commissioners should also ensure that they follow the framework set out in the National Health Service (Procurement, Patient Choice and Competition) (No 2) Regulations 2013. Guidance by Monitor on these regulations is available here. Further background information on this local payment example and how it relates to other areas of Monitor’s work can be found here. www.gov.uk/government/collections/different.
https://www.gov.uk/search/all?keywords=payment+model&order=relevance
Commissioners and providers of mental healthcare need to place greater emphasis on achieving the right outcomes for service users. The use of agreed outcome measures in mental healthcare enables clinicians and providers to have a common vision of how to meet service user needs. It allows key units of measurement to move away from an emphasis on inputs, and offers a language to support care that is more patient-centred.
The inclusion of an outcomes-based component in payment approaches should incentivise providers and commissioners to provide and pay for services that promote better outcomes for patients, rather than better activities or processes. There is good evidence from national and international healthcare systems for a range of benefits to be gained from the inclusion of this component in payments.
Historically, mental healthcare has been paid for using block contracts and data flows have been centred on activity. This has not encouraged a detailed understanding of where and how service user needs are being met. Many providers and commissioners now use the mental healthcare clusters as the sole basis of payment: these group service users with similar care needs and relate payment to components such as a required number of appointments, attendances and specific treatments completed.
Outcomes-based payment draws the attention of all the players in a healthcare system to achieving the target patient outcomes because it rewards co-ordinated care arrangements that deliver those outcomes more efficiently. The approach is based on the assumption the efficiencies of the current healthcare system can be improved, as suggested by evidence from the United States, Valencia in Spain and many other areas. In these areas, payment arrangements combining a fixed core component based on capitation with an outcomes-based component have improved outcomes for service users and transformed the delivery of care (see Appendices 2 and 3 for examples). Evidence indicates that such payment arrangements offer benefits for patients, providers and local mental healthcare systems:
Benefits to patients:
o improved patient experience of care as this care is less fragmented and better co-ordinated
o improved outcomes, such as more time spent living independently at home, reduced acute readmissions and more timely access to care o better information for patients about their care o broader patient choice
Benefits to providers:
o more stable and predictable income, supporting service delivery
o better alignment of patient pathways and care processes with outcomes
o clearer definition from commissioners of what reimbursement will be based on, possibly for a period of several years
o development of a culture of collaboration and integration between providers across the mental health and social care economic system
Benefits to commissioners:
o binding contractual agreements with providers, with real rewards and penalties tied to defined outcomes and performance targets
o improved value for money shown by measurable benefits to patients
o streamlining of the bureaucracy and administration required to manage multiple providers and contracts
System-wide benefits:
o reduced duplication and transaction costs across organisations
o promotion of investment in prevention, quality improvement and working practices that deliver savings and efficiencies over the longer term, where contracts run for a sufficient length of time
o number of key performance indicators (KPIs) reduced to those central to improving patient outcomes.
Forms of contracting that can support co-ordinated approaches to outcomes-based payment
It is possible to link outcomes-based payment to almost any payment arrangement. It is also possible to arrange for service provision with a number of local providers through a range of co-ordinated contractual arrangements. These promote an outcomes-based payment approach that overtly shares common objectives across the system, including outcomes-based payment. Examples of such arrangements in England and elsewhere are:
Prime contractor: a single provider assumes all clinical and financial responsibility for delivering defined patient outcomes. This provider leads the integration of services for patients, sometimes along a whole care pathway, sometimes for a defined patient population, through subcontracts with other providers. Commissioners hold a single contract with the prime contractor. The prime contractor may be an existing provider, a broker or an integrating organisation.
Lead accountable provider: as above, a single provider is accountable for providing a whole care pathway or pathways, or achieving defined outcomes for a defined patient population. Commissioners hold a single contract with this provider, who may subcontract some parts of the pathway or some services. However, in this case, the lead accountable provider retains key accountability for delivery of appropriate, quality care on the pathway (see Section 5 for more details).
Alliance: typically led by commissioners, this contracting mechanism aims to incentivise a number of providers to co-operate to deliver a particular service or an interrelated set of services. Providers enter into linked contracts with commissioners, with the latter evaluating these collectively. Each party maintains its own internal financial controls and shares gain/loss risks with the other commissioners and providers in the alliance.
Joint venture: providers jointly create a new vehicle to facilitate provision of integrated care, but each provider remains independent. The joint venture agreement specifies its nature, responsibilities and governance. Commissioners contract with the joint venture (rather than individual providers) for the delivery of services.
Fully integrated care: as above, commissioners hold a single contract with a single direct or indirect provider of care, but this organisation assumes all responsibility for providing services for an entire care pathway or patient population.
Each of these delivery approaches has its own strengths and weaknesses, which are not explored fully in this document. However, when implementing any of them, commissioners and providers should take care to:
avoid double counting of services, ie ensure that services to be contracted to one or more providers are not contractually covered by another provider
include sufficient incentives in the contracts to encourage better co-ordination of services between all the providers involved; incentives should promote prevention, early intervention and treatment of service users in the lowest intensity care setting that is appropriate for their needs
develop service models capable of delivering co-ordinated services on a larger scale, as well as the mechanisms for recording and sharing the data necessary for managing the delivery of larger, longer-term contracts and monitoring progress on outcomes.
The lead accountable provider model
In this model, commissioners have a single contract with one provider organisation – the lead provider – which may have one of two broad types of accountability.
For a defined population: a lead provider or group of providers is accountable for managing an agreed range of health and social care needs and achieving agreed outcomes for a defined population. The contract may apply to the care for a local population within a specific geography or to the care for a clearly defined segment of this population.
For a defined pathway: the provider(s) is accountable for service user outcomes from the commissioned single ‘pathway’ of care for a particular condition over a defined period of time.
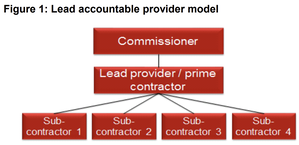
With either type of accountability, the lead provider organises the other providers of services that are needed by either the population or the care pathway, and is responsible for subcontracting the delivery of their services (see Figure 1). In the existing contractual legal framework, the lead provider cannot decommission subcontracted providers without the approval of the commissioners. Also, an underpinning principle is that service users are closely involved with commissioners and providers in defining the desired outcomes of the services.
The payment arrangement in the contract links a share of the payment made to the lead accountable provider to achievement of defined outcomes. In practice, this arrangement places both accountability for patient outcomes and control over how patient services are organised with the lead accountable provider. It also shifts a degree of financial risk to that provider.
The payment arrangement in the contract links a share of the payment made to the lead accountable provider to achievement of defined outcomes. In practice, this arrangement places both accountability for patient outcomes and control over how patient services are organised with the lead accountable provider. It also shifts a degree of financial risk to that provider.

The local payment approach comprises:
1. a fixed core component
2. an outcomes-based incentive payment
3. a component that shares financial gains or losses between providers and commissioners, relative to the value of the agreed total payment to the provider.
1. a fixed core component
2. an outcomes-based incentive payment
3. a component that shares financial gains or losses between providers and commissioners, relative to the value of the agreed total payment to the provider.
The first and second components are based on capitation: the risk share component may or may not be calculated within the same capitated budget. Depending on local circumstances and the intended care model, local commissioners and providers (including subcontractors) may want to consider:
the appropriate weighting or emphasis to attach to each payment component (note the percentages below have been chosen for illustrative purposes only; in practice the share of payment linked to outcomes may be smaller and the core payment larger)
whether or not the total capitated budget will be spread across all three components or cover only the core and outcomes components (as in the example above). The option chosen may affect the way parties entering into the payment agreement react to the incentives. For example, if the risk share element is taken from the capitated budget, providers may feel their capitated budget will be reduced if they achieve savings, which could lower staff morale and act as a barrier to innovation and change
the appropriate weighting or emphasis to attach to each payment component (note the percentages below have been chosen for illustrative purposes only; in practice the share of payment linked to outcomes may be smaller and the core payment larger)
whether or not the total capitated budget will be spread across all three components or cover only the core and outcomes components (as in the example above). The option chosen may affect the way parties entering into the payment agreement react to the incentives. For example, if the risk share element is taken from the capitated budget, providers may feel their capitated budget will be reduced if they achieve savings, which could lower staff morale and act as a barrier to innovation and change

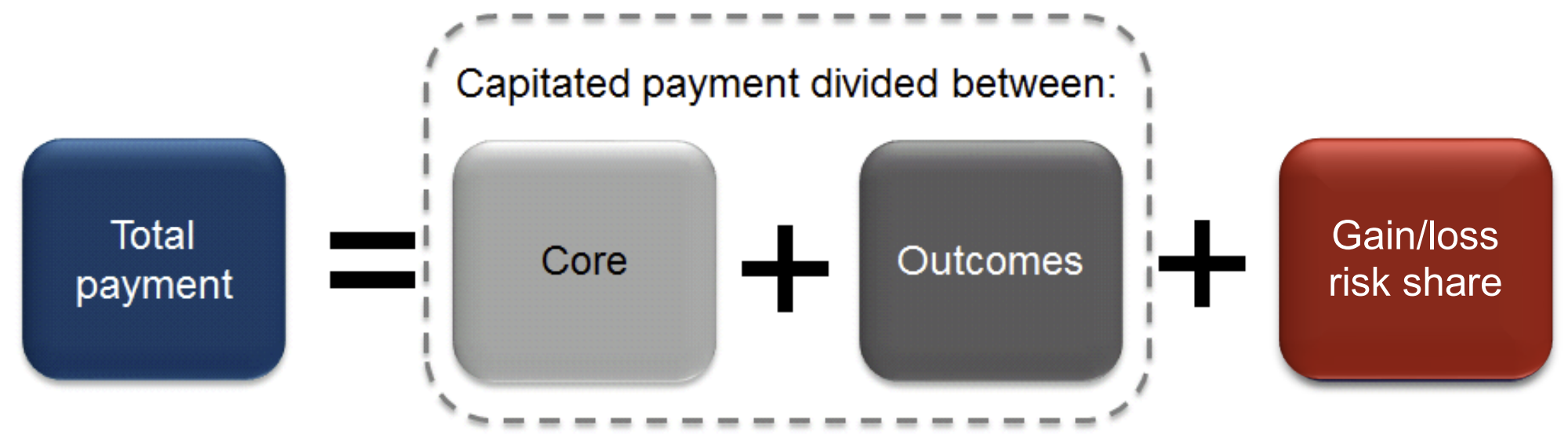
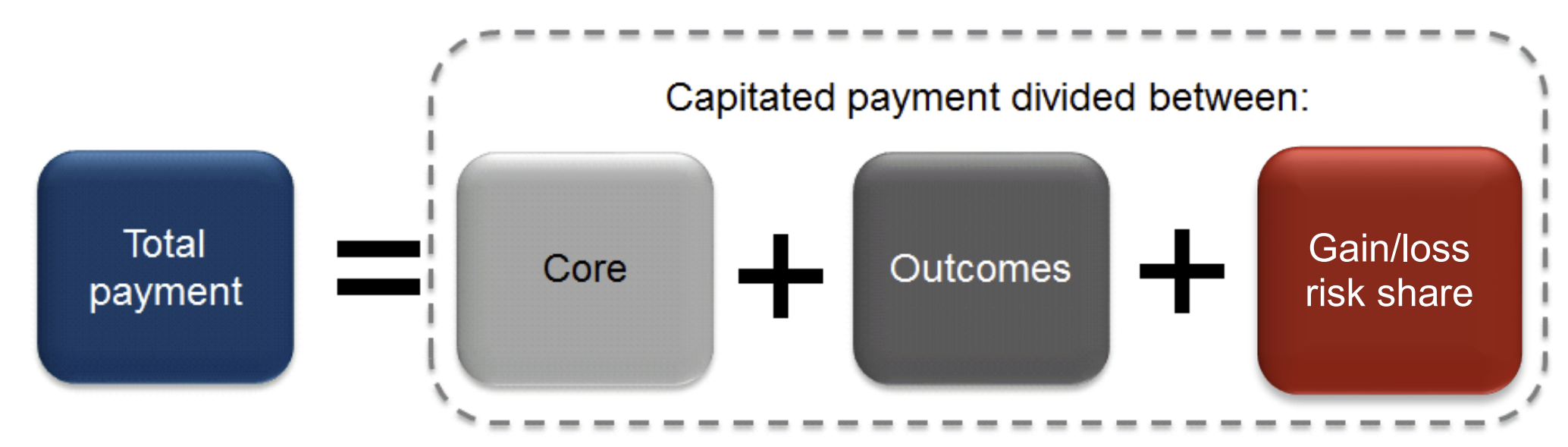
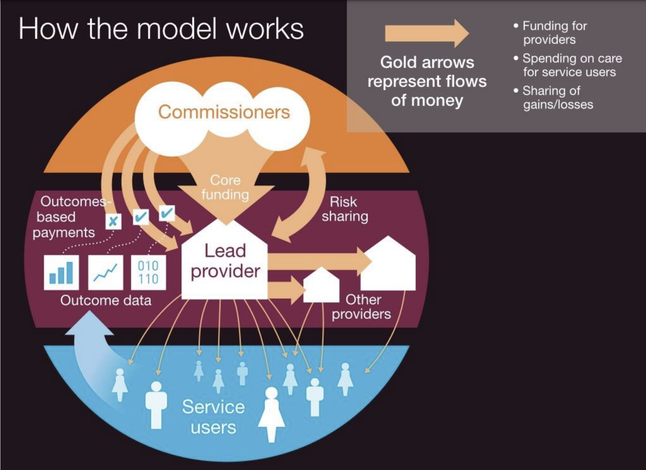
Overview of capitated outcomes-based payment with a gain/loss risk share component
To develop this payment approach, commissioners and providers need to agree a total capitated budget. In principle, payment based on capitation means the provider is paid a lump sum per person for meeting the care needs of a defined target population. The size of that lump sum is (i) determined by calculating the total efficient cost of inputs required to deliver that population’s care needs and (ii) dividing this amount by the number of people in the defined population. People in the defined population will have different levels of need, requiring different levels of resources. So, capitated budgets need to be weighted or risk adjusted to take these differences into account. Detailed information on developing capitated payments can be found in the published capitation payment example.
Overview of capitated outcomes-based payment with a gain/loss risk share component
To develop this payment approach, commissioners and providers need to agree a total capitated budget. In principle, payment based on capitation means the provider is paid a lump sum per person for meeting the care needs of a defined target population. The size of that lump sum is (i) determined by calculating the total efficient cost of inputs required to deliver that population’s care needs and (ii) dividing this amount by the number of people in the defined population. People in the defined population will have different levels of need, requiring different levels of resources. So, capitated budgets need to be weighted or risk adjusted to take these differences into account. Detailed information on developing capitated payments can be found in the published capitation payment example.
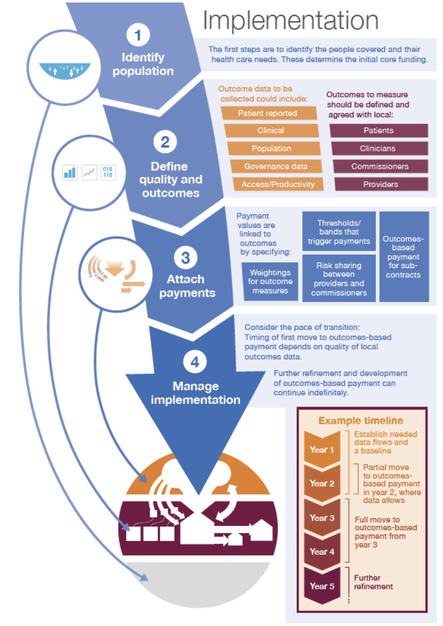
Overview of the transition process
